

Risk of adverse gastrointestinal outcomes in patients taking cyclo-oxygenase-2 inhibitors or conventional non-steroidal anti-inflammatory drugs: population based nested case-control analysis
- PMID: 16322018
- PMCID: PMC1298853
- DOI: 10.1136/bmj.331.7528.1310
Risk of adverse gastrointestinal outcomes in patients taking cyclo-oxygenase-2 inhibitors or conventional non-steroidal anti-inflammatory drugs: population based nested case-control analysis
Abstract
Objective: To determine the risk of an adverse upper gastrointestinal event in patients taking different cyclo-oxygenase-2 inhibitors compared with non-selective non-steroidal anti-inflammatory drugs.
Design: Nested case-control study.
Setting: 367 general practices contributing to the UK QRESEARCH database, spread throughout every strategic health authority and each health board in England, Wales, and Scotland.
Participants: Patients aged 25 or more with a first ever diagnosis of an adverse upper gastrointestinal event (peptic ulcer or haematemesis) between 1 August 2000 and 31 July 2004 and up to 10 controls per case matched for age, sex, calendar time, and practice.
Main outcome measures: Unadjusted and adjusted odds ratios for adverse upper gastrointestinal events associated with celecoxib, rofecoxib, ibuprofen, diclofenac, naproxen, other selective and non-selective non-steroidal anti-inflammatory drugs, and aspirin.
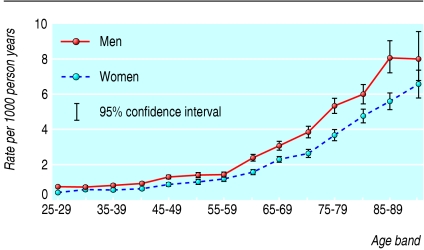
Results: The incidence of adverse upper gastrointestinal events was 1.36 per 1000 person years (95% confidence interval 1.34 to 1.39). We identified 9407 incident cases and 88 867 matched controls. Increased risks of adverse gastrointestinal events were associated with current use of cyclo-oxygenase-2 inhibitors and with conventional non-steroidal anti-inflammatory drugs. Risks were reduced after adjustment for confounders but remained significantly increased for naproxen (adjusted odds ratio 2.12, 95% confidence interval 1.73 to 2.58), diclofenac (1.96, 1.78 to 2.15), and rofecoxib (1.56, 1.30 to 1.87) but not for current use of celecoxib (1.11, 0.87 to 1.41). We found clinically important interactions with current use of ulcer healing drugs that removed the increased risks for adverse gastrointestinal events for all groups of non-steroidal anti-inflammatory drugs except diclofenac, which still had an increased odds ratio (1.49, 1.26 to 1.76).
Conclusion: No consistent evidence was found of enhanced safety against gastrointestinal events with any of the new cyclo-oxygenase-2 inhibitors compared with non-selective non-steroidal anti-inflammatory drugs. The use of ulcer healing drugs reduced the increased risk of adverse gastrointestinal outcomes with all groups of non-steroidal anti-inflammatory drugs, but for diclofenac the increased risk remained significant.
Figures
Comment in
-
Risk of gastrointestinal effects with COX-2 inhibitors and NSAIDs: study conclusions do not reflect findings for celecoxib.BMJ. 2005 Dec 17;331(7530):1473-4. doi: 10.1136/bmj.331.7530.1473-d. BMJ. 2005. PMID: 16356991 Free PMC article. No abstract available.
-
Risk of gastrointestinal effects with COX-2 inhibitors and NSAIDs: what does evidence from randomised trials show about celecoxib?BMJ. 2005 Dec 17;331(7530):1474-5. doi: 10.1136/bmj.331.7530.1474-c. BMJ. 2005. PMID: 16356996 Free PMC article. No abstract available.
-
Risk of gastrointestinal effects with COX-2 inhibitors and NSAIDs: COX-2 inhibitors were thought of as a safe option.BMJ. 2005 Dec 17;331(7530):1474. doi: 10.1136/bmj.331.7530.1474-b. BMJ. 2005. PMID: 16356997 Free PMC article. No abstract available.
-
Risk of gastrointestinal effects with COX-2 inhibitors and NSAIDs: why were patients at major risk excluded?BMJ. 2005 Dec 17;331(7530):1474. doi: 10.1136/bmj.331.7530.1474-a. BMJ. 2005. PMID: 16356998 Free PMC article. No abstract available.
-
Risk of gastrointestinal effects with COX-2 inhibitors and NSAIDs: how strong is the evidence?BMJ. 2005 Dec 17;331(7530):1474. doi: 10.1136/bmj.331.7530.1474. BMJ. 2005. PMID: 16356999 Free PMC article. No abstract available.
-
Life without COX 2 inhibitors: risks and benefits are determined by dose and potency.BMJ. 2006 Jun 17;332(7555):1451-2. doi: 10.1136/bmj.332.7555.1451-b. BMJ. 2006. PMID: 16777893 Free PMC article. No abstract available.
References
-
- National Institute for Clinical Excellence. The clinical effectiveness and cost effectiveness of celecoxib, rofecoxib, meloxicam and etodolac (cox-II inhibitors) for rheumatoid arthritis and osteoarthritis. London: NICE, 2000.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical