

beta-Adrenergic receptor polymorphisms and response to salmeterol
- PMID: 16322642
- PMCID: PMC2662935
- DOI: 10.1164/rccm.200509-1519OC
beta-Adrenergic receptor polymorphisms and response to salmeterol
Abstract
Rationale: Several studies suggest that patients with asthma who are homozygous for arginine at the 16th position of the beta2-adrenergic receptor may not benefit from short-acting beta-agonists.
Objectives: We investigated whether such genotype-specific effects occur when patients are treated with long-acting beta-agonists and whether such effects are modified by concurrent inhaled corticosteroid (ICS) use.
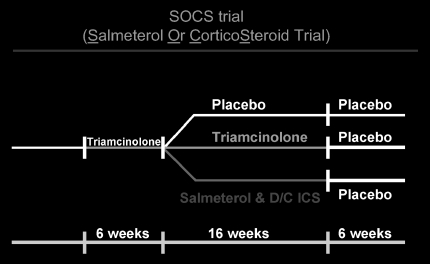
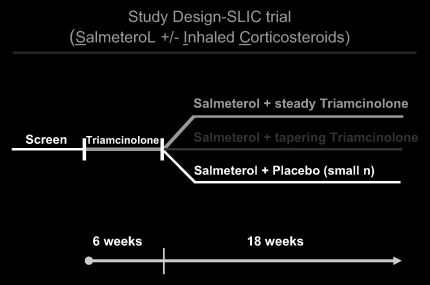
Methods: We compared salmeterol response in patients with asthma homozygous for arginine at B16 (B16Arg/Arg) with those homozygous for glycine at B16 (B16Gly/Gly) in two separate cohorts. In the first, subjects were randomized to regular therapy with salmeterol while simultaneously discontinuing ICS therapy. In the second, subjects were randomized to regular therapy with salmeterol while continuing concomitant ICS.
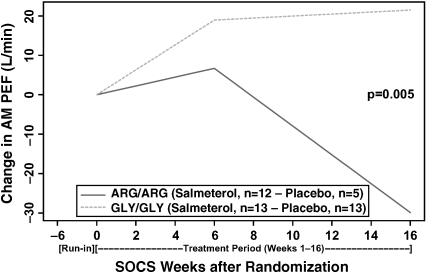
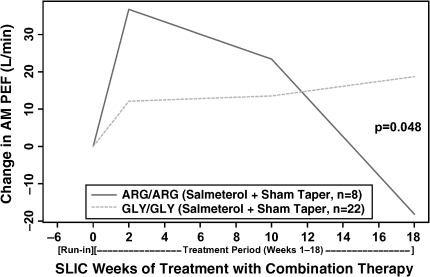
Results: In both trials, B16Arg/Arg subjects did not benefit compared with B16Gly/Gly subjects after salmeterol was initiated. In the first cohort, compared with placebo, the addition of salmeterol was associated with a 51.4 L/min lower A.M. peak expiratory flow (PEF; p = 0.005) in B16Arg/Arg subjects(salmeterol, n = 12; placebo, n = 5) as compared with B16Gly/Gly subjects (salmeterol, n = 13; placebo, n = 13). In the second cohort, B16Arg/Arg subjects treated with salmeterol and ICS concurrently (n = 8) had a lower A.M. PEF (36.8 L/min difference, p = 0.048) than B16Gly/Gly subjects (n = 22) treated with the same regimen. In addition, B16 Arg/Arg subjects in the second cohort had lower FEV1 (0.42 L, p = 0.003), increased symptom scores (0.2 units, p = 0.034), and increased albuterol rescue use (0.95 puffs/d, p = 0.004) compared with B16Gly/Gly subjects.
Conclusions: Relative to B16Gly/Gly patients with asthma, B16Arg/Arg patients with asthma may have an impaired therapeutic response to salmeterol in either the absence or presence of concurrent ICS use. Investigation of alternate treatment strategies may benefit this group.
Figures
Comment in
-
beta-Adrenoceptor polymorphisms: focus moves to long-acting beta-agonists.Am J Respir Crit Care Med. 2006 Mar 1;173(5):473-4. doi: 10.1164/rccm.2512005. Am J Respir Crit Care Med. 2006. PMID: 16493161 No abstract available.
References
-
- Nelson HS. Drug therapy: beta-adrenergic bronchodilators. N Engl J Med 1995;333:499–506. - PubMed
-
- Sears MR, Taylor DR, Print CG, Lake DC, Li QQ, Flannery EM, Yates DM, Lucas MK, Herbison GP. Regular inhaled beta-agonist treatment in bronchial asthma. Lancet 1990;336:1391–1396. - PubMed
-
- Drazen JM, Israel E, Boushey HA, Chinchilli VM, Fahy JV, Fish JE, Lazarus SC, Lemanske RF, Martin RJ, Peters SP, et al. Comparison of regularly scheduled with as-needed use of albuterol in mild asthma. N Engl J Med 1996;335:841–847. - PubMed
-
- Sears MR. Is the routine use of inhaled beta-adrenergic agonists appropriate in asthma treatment? No. Am J Respir Crit Care Med 1995;151:600–601. - PubMed
-
- Wanner A. Is the routine use of inhaled beta-adrenergic agonists appropriate in asthma treatment? Yes. Am J Respir Crit Care Med 1995;151:597–599. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
