

Hospital volume and mortality after pancreatic resection: a systematic review and an evaluation of intervention in the Netherlands
- PMID: 16327488
- PMCID: PMC1409869
- DOI: 10.1097/01.sla.0000188462.00249.36
Hospital volume and mortality after pancreatic resection: a systematic review and an evaluation of intervention in the Netherlands
Abstract
Objectives: To evaluate the best available evidence on volume-outcome effect of pancreatic surgery by a systematic review of the existing data and to determine the impact of the ongoing plea for centralization in The Netherlands.
Summary background data: Centralization of pancreatic resection (PR) is still under debate. The reported impact of hospital volume on the mortality rate after PR varies. Since 1994, there has been a continuous plea for centralization of PR in The Netherlands, based on repetitive analysis of the volume-outcome effect.
Methods: A systematic search for studies comparing hospital mortality rates after PR between high- and low-volume hospitals was used. Studies were reviewed independently for design features, inclusion and exclusion criteria, cutoff values for high and low volume, and outcome. Primary outcome measure was hospital or 30-day mortality. Data were obtained from the Dutch nationwide registry on the outcome of PR from 1994 to 2004. Hospitals were divided into 4 volume categories based on the number of PRs performed per year. Interventions and their effect on mortality rates and centralization were analyzed.
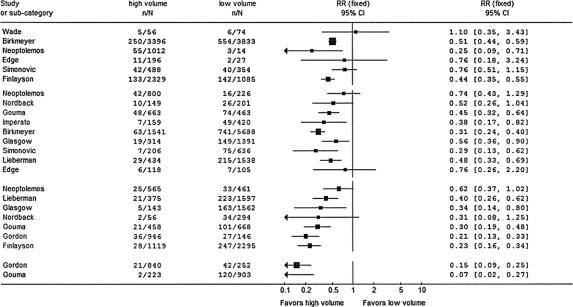
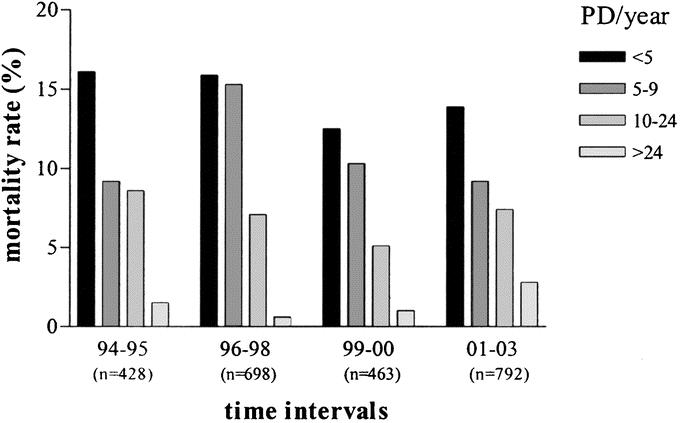
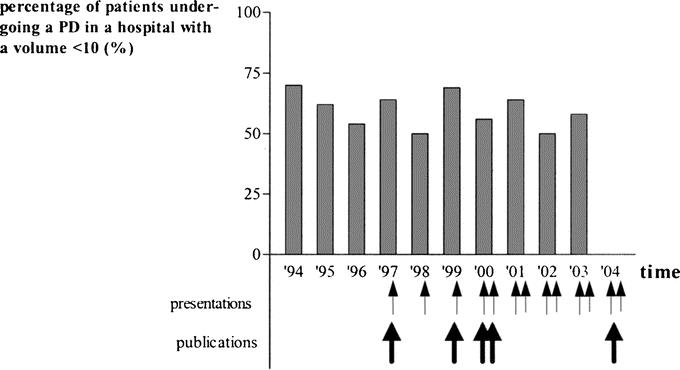
Results: Twelve observational studies with a total of 19,688 patients were included. The studies were too heterogeneous to allow a meta-analysis; therefore, a qualitative analysis was performed. The relative risk of dying in a high-volume hospital compared with a low-volume hospital was between 0.07 and 0.76, and was inversely proportional to the volume cutoff values arbitrarily defined. In 5 evaluations within a decade, hospital mortality rates were between 13.8% and 16.5% in hospitals with less than 5 PRs per year, whereas hospital mortality rates were between 0% and 3.5% in hospitals with more than 24 PRs per year. Despite the repetitive plea for centralization, no effect was seen. During 2001, 2002, and 2003, 454 of 792 (57.3%) patients underwent surgery in hospitals with a volume of less than 10 PRs per year, compared with 280 of 428 (65.4%) patients between 1994 and 1996.
Conclusions: The data on hospital volume and mortality after PR are too heterogeneous to perform a meta-analysis, but a systematic review shows convincing evidence of an inverse relation between hospital volume and mortality and enforces the plea for centralization. The 10-year lasting plea for centralization among the surgical community did not result in a reduction of the mortality rate after PR or change in the referral pattern in The Netherlands.
Figures
Republished in
-
[Centralisation of pancreatic resection: a systematic review and evaluation in the Netherlands].Ned Tijdschr Geneeskd. 2006 Apr 8;150(14):791-8. Ned Tijdschr Geneeskd. 2006. PMID: 16649399 Dutch.
References
-
- Kuhlmann KF, de Castro SM, Wesseling JG, et al. Surgical treatment of pancreatic adenocarcinoma; actual survival and prognostic factors in 343 patients. Eur J Cancer. 2004;40:549–558. - PubMed
-
- Millikan KW, Deziel DJ, Silverstein JC, et al. Prognostic factors associated with resectable adenocarcinoma of the head of the pancreas. Am Surg. 1999;65:618–623; discussion 623–624. - PubMed
-
- Sohn TA, Yeo CJ, Cameron JL, et al. Resected adenocarcinoma of the pancreas-616 patients: results, outcomes, and prognostic indicators. J Gastrointest Surg. 2000;4:567–579. - PubMed
-
- Neoptolemos JP, Russell RC, Bramhall S, et al. Low mortality following resection for pancreatic and periampullary tumours in 1026 patients: UK survey of specialist pancreatic units. UK Pancreatic Cancer Group. Br J Surg. 1997;84:1370–1376. - PubMed
-
- Bramhall SR, Allum WH, Jones AG, et al. Treatment and survival in 13,560 patients with pancreatic cancer, and incidence of the disease, in the West Midlands: an epidemiological study. Br J Surg. 1995;82:111–115. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
