

CD4(+)CD25high regulatory T cells increase with tumor stage in patients with gastric and esophageal cancers
- PMID: 16328385
- PMCID: PMC11030626
- DOI: 10.1007/s00262-005-0092-8
CD4(+)CD25high regulatory T cells increase with tumor stage in patients with gastric and esophageal cancers
Abstract
Purpose: Regulatory T cells (T regs) can inhibit immune responses mediated by T cells. It has been shown that there is an increased proportion of T regs in several different human malignancies, although the actual mechanism remains unclear. In the present study, we evaluated the prevalence of CD4(+)CD25high T regs in PBMCs from patients with gastric and esophageal cancers in relation to the clinical outcome.
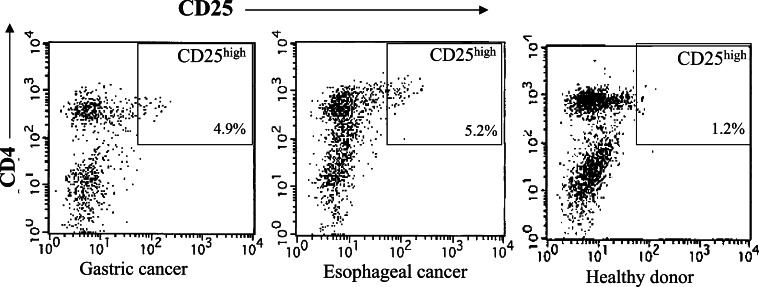
Methods: PBMCs in 72 patients with gastric cancer and 42 patients with esophageal cancer were evaluated for the proportion of CD4(+)CD25high T cells, as a percentage of the total CD4(+) cells, by flow cytometric analysis with triple-color staining. Actuarial overall survival rates of the patients were analyzed by the Kaplan-Meier method.
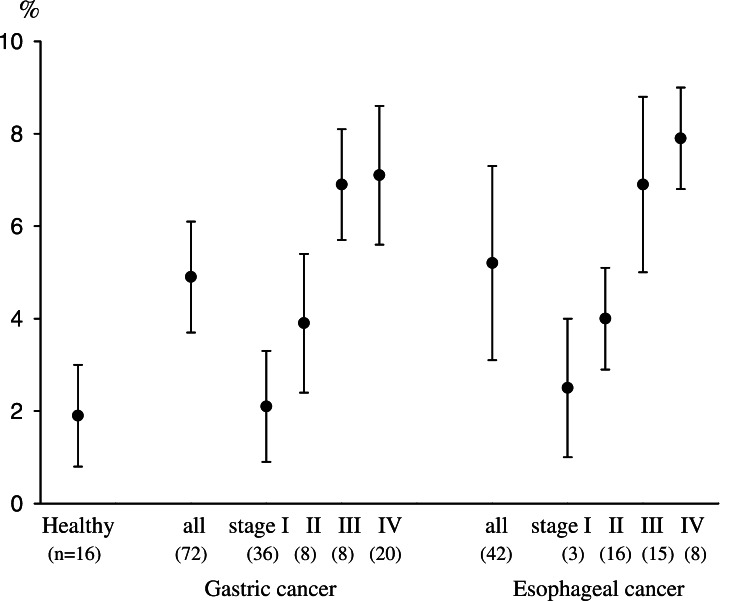
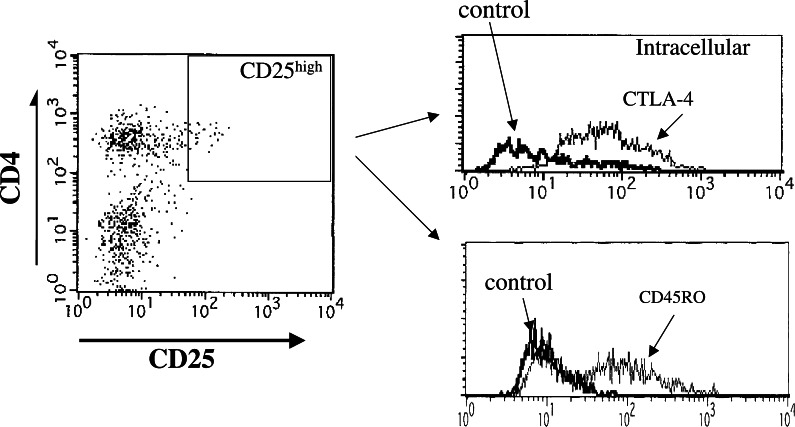
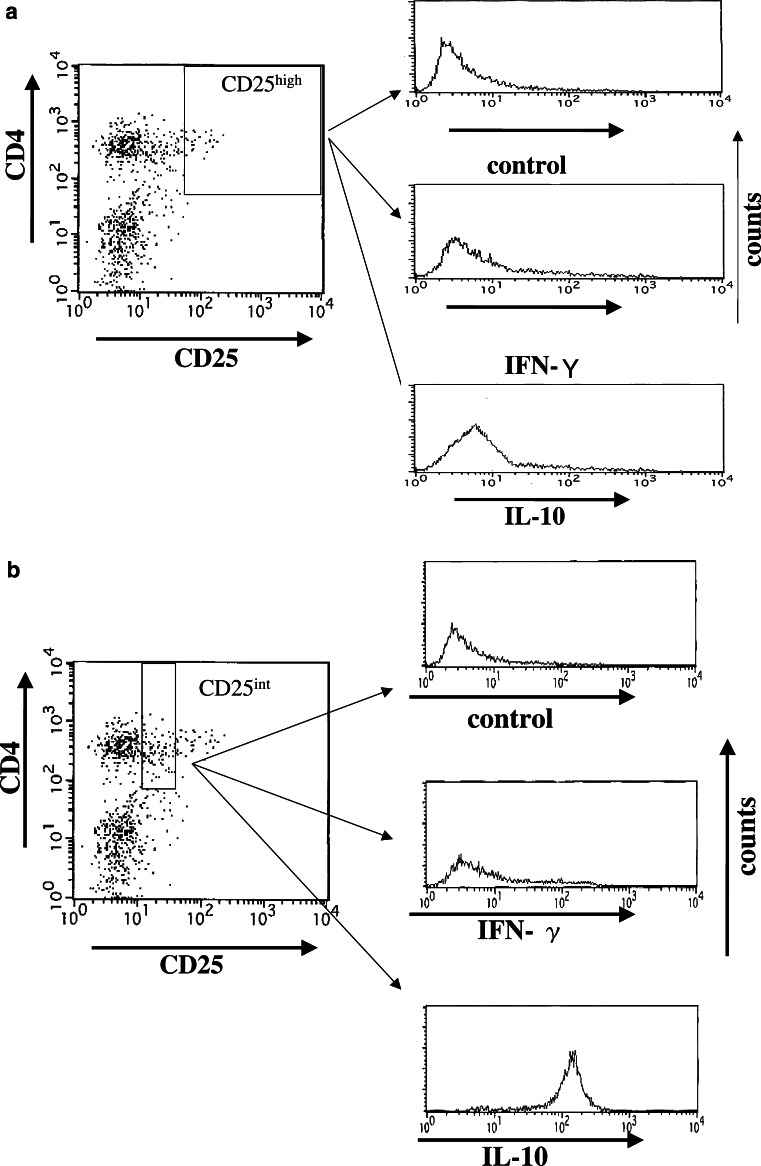
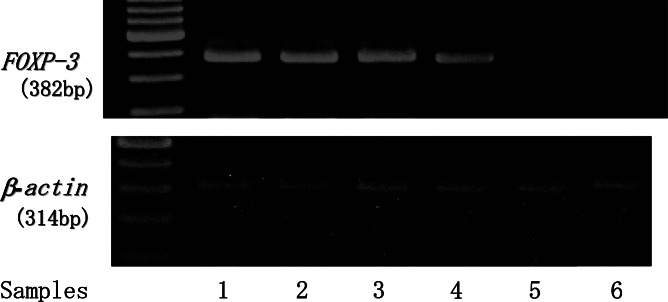
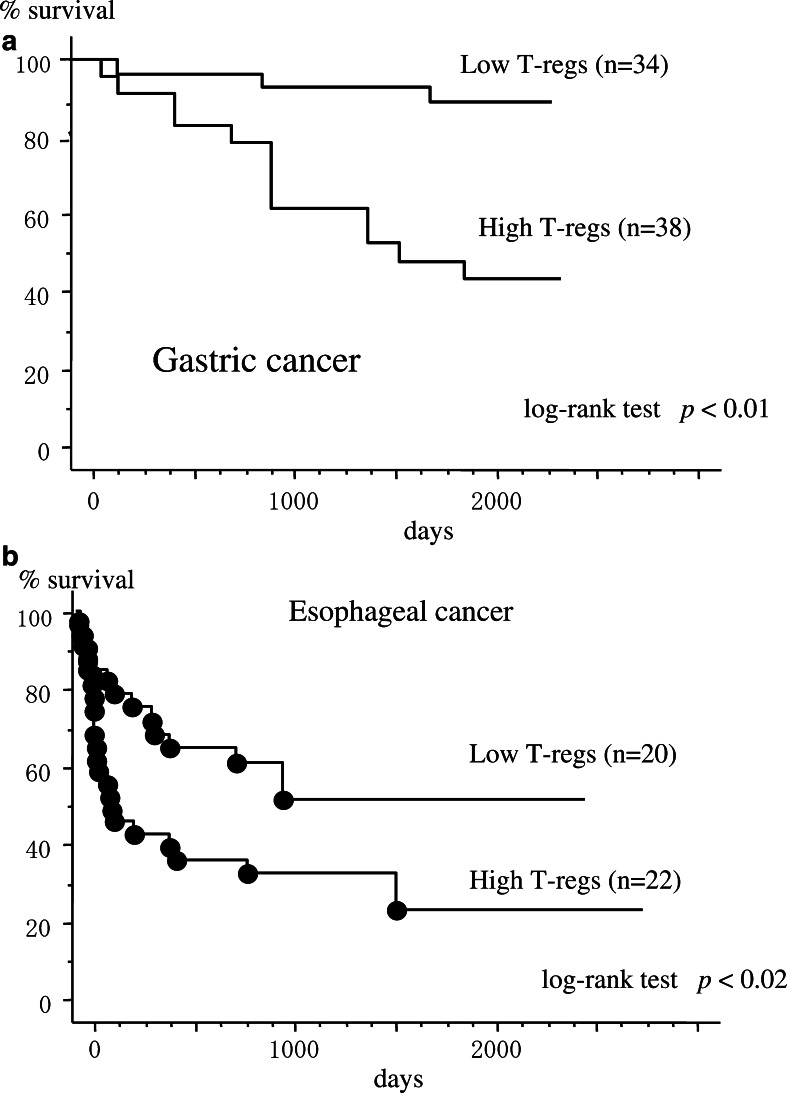
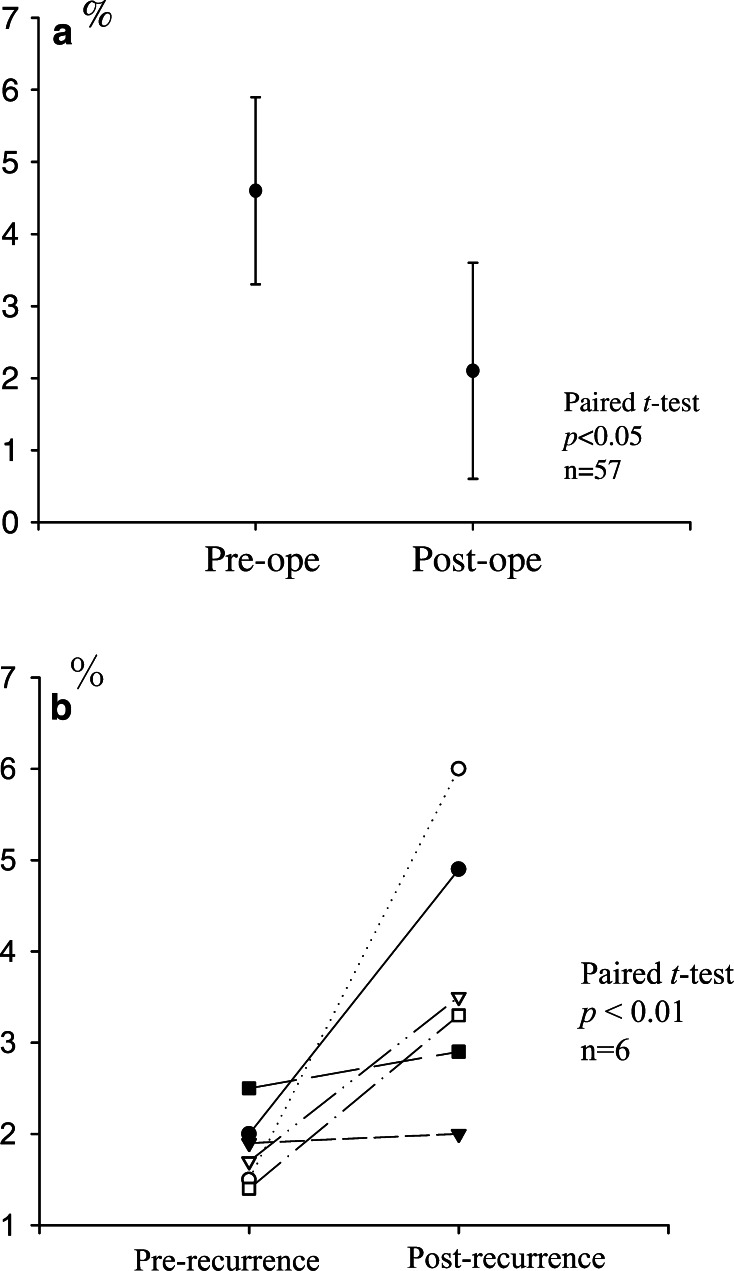
Results: The percentages of CD4(+)CD25high T cells for cases of gastric cancer (4.9+/-1.2%) and esophageal cancer (5.2+/-2.1%) were significantly higher than those for healthy donors (1.9+/-1.1%, P<0.01). There were significant differences in the prevalence of CD4(+)CD25high T cells between the early and advanced disease stages, both in gastric cancer (stage I vs. III, P<0.05; stage I vs. IV, P<0.05) and esophageal cancer (stage I vs. IV, P<0.05). The patients with a high proportion of CD4(+)CD25high T cells showed poorer survival rates in comparison to those with a low proportion, in both gastric and esophageal cancers. After patients received curative resections of gastric cancers (n=57), the increased proportions of CD4(+)CD25high T cells were significantly reduced, and the levels were almost equal to those in normal healthy donors. In addition, studies of gastric cancer patients with postoperative recurrent tumors (n=6) revealed that the prevalence of CD4(+)CD25high T cells individually increased compared to 2 months after the operations. CD4(+)CD25high T cells expressed FOXP3 mRNA and had abundant CD45RO and intracellular CTLA-4 molecules.
Conclusions: These results strongly suggest that tumor-related factors induce and expand CD4(+)CD25high T regs.
Figures
References
-
- Sakaguchi S, Sakaguchi N, Asano M, Itoh M, Toda M. Immunologic self-tolerance maintained by activated T cells expressing IL-2 receptor alpha-chains (CD25). Breakdown of a single mechanism of self-tolerance causes various autoimmune diseases. J Immunol. 1995;155:1151–1164. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
