

Long-term outcomes in patients with metastatic melanoma vaccinated with melanoma peptide-pulsed CD34(+) progenitor-derived dendritic cells
- PMID: 16331519
- PMCID: PMC11030596
- DOI: 10.1007/s00262-005-0106-6
Long-term outcomes in patients with metastatic melanoma vaccinated with melanoma peptide-pulsed CD34(+) progenitor-derived dendritic cells
Abstract
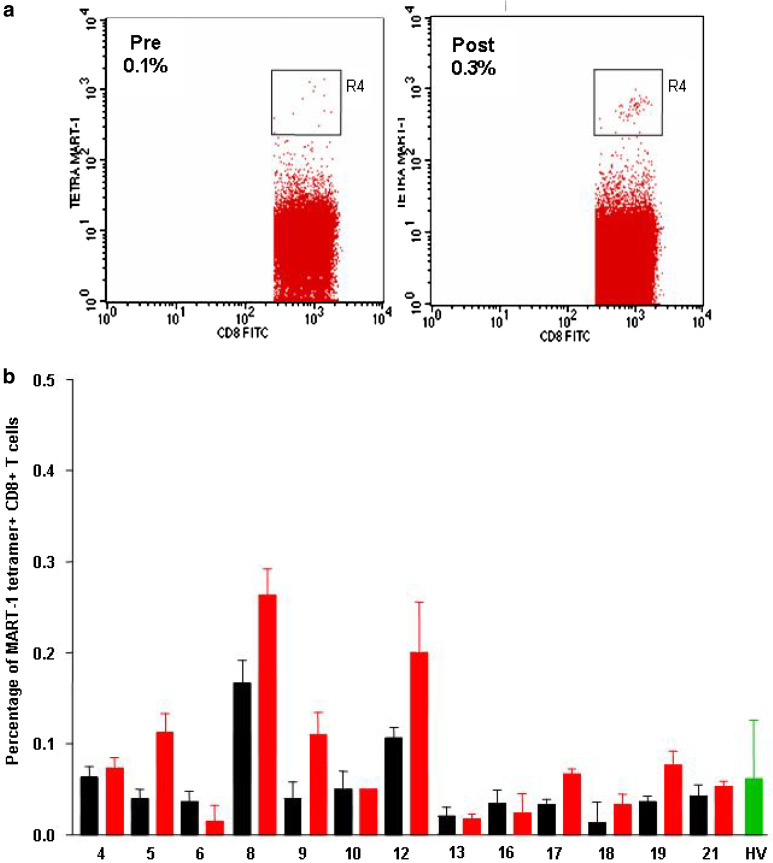
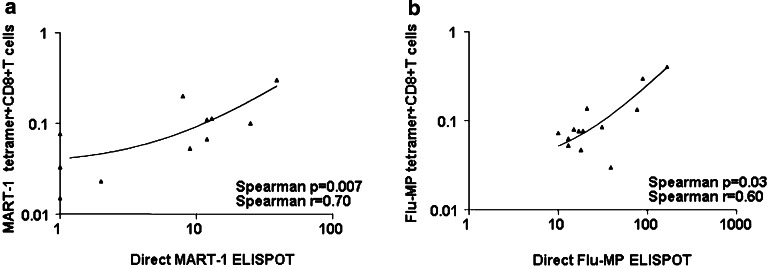
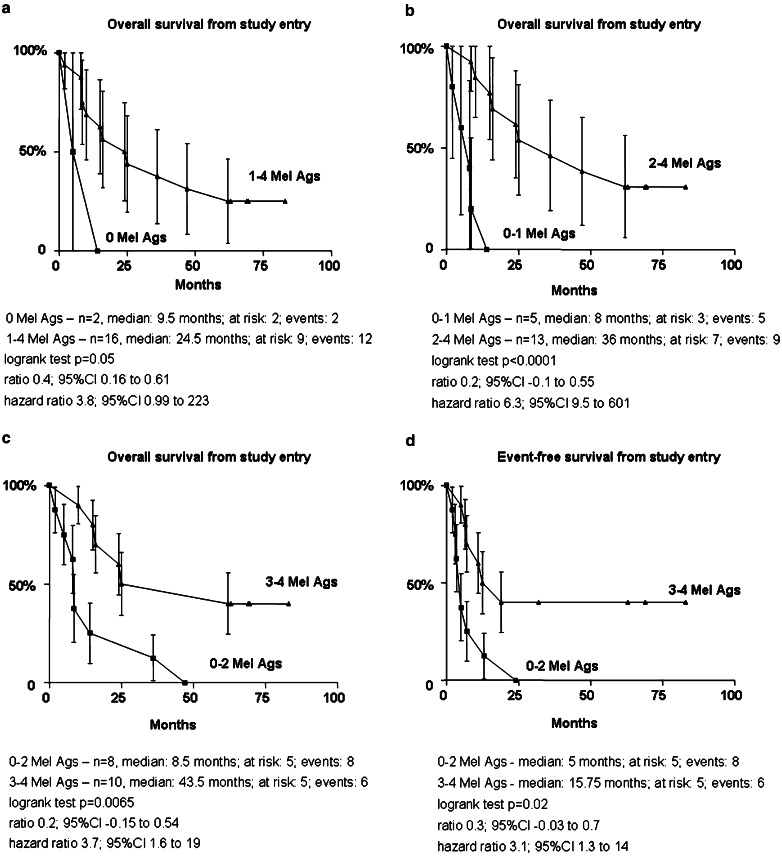
Between March 1999 and May 2000, 18 HLA-A*0201(+) patients with metastatic melanoma were enrolled in a phase I trial using a dendritic cell (DC) vaccine generated by culturing CD34(+) hematopoietic progenitors. This vaccine includes Langerhans cells. The DC vaccine was loaded with four melanoma peptides (MART-1/MelanA, tyrosinase, MAGE-3, and gp100), Influenza matrix peptide (Flu-MP), and keyhole limpet hemocyanin (KLH). Ten patients received eight vaccinations, one patient received six vaccinations, one patient received five vaccinations, and six patients received four vaccinations. Peptide-specific immunity was measured by IFN-gamma production and tetramer staining in blood mononuclear cells. The estimated median overall survival was 20 months (range: 2-83), and the median event-free survival was 7 months (range: 2-83). As of August 2005, four patients are alive (three patients had M1a disease and one patient had M1c disease). Three of them have had no additional therapy since trial completion; two of them had solitary lymph node metastasis, and one patient had liver metastasis. Patients who survived longer were those who mounted melanoma peptide-specific immunity to at least two melanoma peptides. The present results therefore justify the design of larger follow-up studies to assess the immunological and clinical outcomes in patients with metastatic melanoma vaccinated with peptide-pulsed CD34-derived DCs.
Figures
References
-
- Manola J, Atkins M, Ibrahim J, Kirkwood J. Prognostic factors in metastatic melanoma: a pooled analysis of Eastern Cooperative Oncology Group trials. J Clin Oncol. 2000;18:3782–3793. - PubMed
-
- Balch CM, Buzaid AC, Soong SJ, Atkins MB, Cascinelli N, Coit DG, Fleming ID, Gershenwald JE, Houghton A, Jr, Kirkwood JM, McMasters KM, Mihm MF, Morton DL, Reintgen DS, Ross MI, Sober A, Thompson JA, Thompson JF. Final version of the American Joint Committee on Cancer staging system for cutaneous melanoma. J Clin Oncol. 2001;19:3635–3648. - PubMed
-
- Balch C, Soong S, Thompson J. The natural history of melanoma and factors predicting outcome. In: Thompson JF, Morton DL, Kroon BB, editors. Textbook of melanoma. London and New York: Martin Dunitz; 2004. pp. 181–198.
-
- Lotze M, Dallal R, kirkwood J, Flickinger J. Cutaneous melanoma. In: DeVita VT, Hellman S, Rosenberg SA, editors. Cancer: principles and practice of oncology. 6. Philadelphia: LWW; 2001. pp. 2012–2069.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
