

The break-even point: when medical advances are less important than improving the fidelity with which they are delivered
- PMID: 16338919
- PMCID: PMC1466946
- DOI: 10.1370/afm.406
The break-even point: when medical advances are less important than improving the fidelity with which they are delivered
Abstract
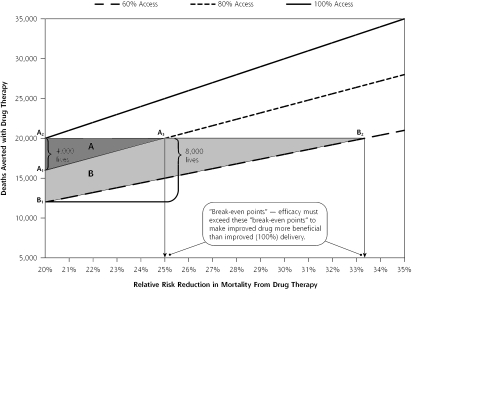
Society invests billions of dollars in the development of new drugs and technologies but comparatively little in the fidelity of health care, that is, improving systems to ensure the delivery of care to all patients in need. Using mathematical arguments and a nomogram, we demonstrate that technological advances must yield dramatic, often unrealistic increases in efficacy to do more good than could be accomplished by improving fidelity. In 2 examples (the development of anti-platelet agents and statins), we show that enhanced efficacy failed to achieve the health gains that would have occurred by delivering older agents to all eligible patients. Society's huge investment in technological innovations that only modestly improve efficacy, by consuming resources needed for improved delivery of care, may cost more lives than it saves. The misalignment of priorities is driven partly by the commercial interests of industry and by the public's appetite for technological breakthroughs, but health outcomes ultimately suffer. Health, economic, and moral arguments make the case for spending less on technological advances and more on improving systems for delivering care.
Figures
Comment in
-
Doing things better vs doing better things.Ann Fam Med. 2005 Nov-Dec;3(6):483-5. doi: 10.1370/afm.407. Ann Fam Med. 2005. PMID: 16338909 Free PMC article. No abstract available.
-
Misaligned incentives in America's health: who's minding the store?Ann Fam Med. 2005 Nov-Dec;3(6):485-7. doi: 10.1370/afm.408. Ann Fam Med. 2005. PMID: 16338910 Free PMC article. No abstract available.
References
-
- McGlynn EA, Asch SM, Adams J, et al. The quality of health care delivered to adults in the United States. N Engl J Med. 2003;348:2635–2645. - PubMed
-
- Smedley BD, Stith AY, Nelson AR, eds. Committee on Understanding and Eliminating Racial and Ethnic Disparities in Health Care BoHSP, Institute of Medicine. Unequal Treatment: Confronting Racial and Ethnic Disparities in Health Care. Washington, DC: National Academies Press; 2003. - PubMed
-
- Von Korff M, Gruman J, Schaefer J, Curry SJ, Wagner EH. Collaborative management of chronic illness. Ann Intern Med. 1997;127:1097–1102. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical