

The Hospital Anxiety and Depression Rating Scale: a cross-sectional study of psychometrics and case finding abilities in general practice
- PMID: 16351733
- PMCID: PMC1343544
- DOI: 10.1186/1471-244X-5-46
The Hospital Anxiety and Depression Rating Scale: a cross-sectional study of psychometrics and case finding abilities in general practice
Abstract
Background: General practitioners' (GPs) diagnostic skills lead to underidentification of generalized anxiety disorders (GAD) and major depressive episodes (MDE). Supplement of brief questionnaires could improve the diagnostic accuracy of GPs for these common mental disorders. The aims of this study were to examine the usefulness of The Hospital Anxiety and Depression Rating Scale (HADS) for GPs by: 1) Examining its psychometrics in the GPs' setting; 2) Testing its case-finding properties compared to patient-rated GAD and MDE (DSM-IV); and 3) Comparing its case finding abilities to that of the GPs using Clinical Global Impression-Severity (CGI-S) rating.
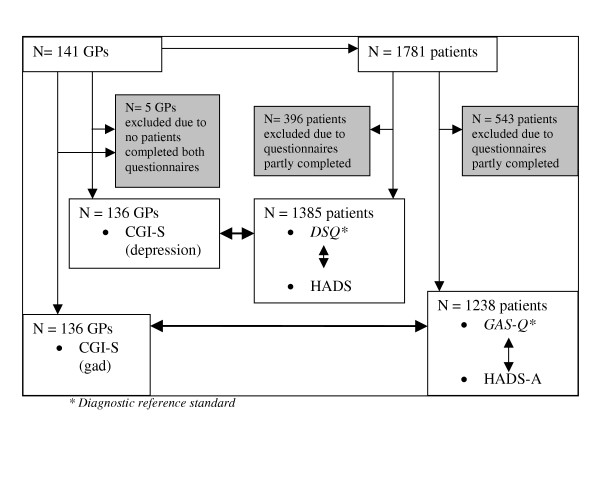
Methods: In a cross-sectional survey study 1,781 patients in three consecutive days in September 2001 attended 141 GPs geographically spread in Norway. Sensitivity, specificity, optimal cut off score, and Area under the curve (AUC) for the HADS and the CGI-S were calculated with Generalized Anxiety Questionnaire (GAS-Q) as reference standard for GAD, and Depression Screening Questionnaire (DSQ) for MDE.
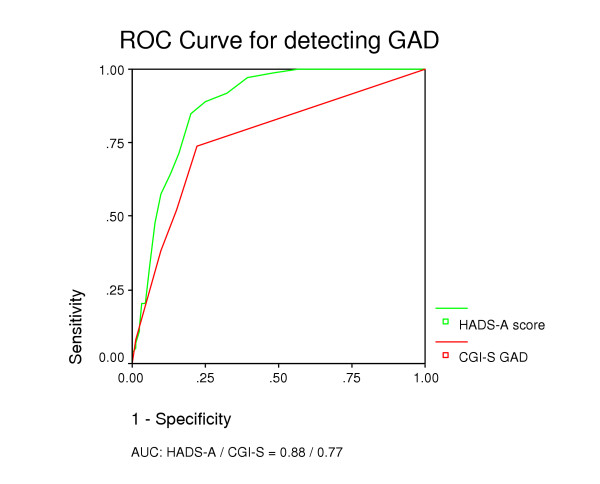
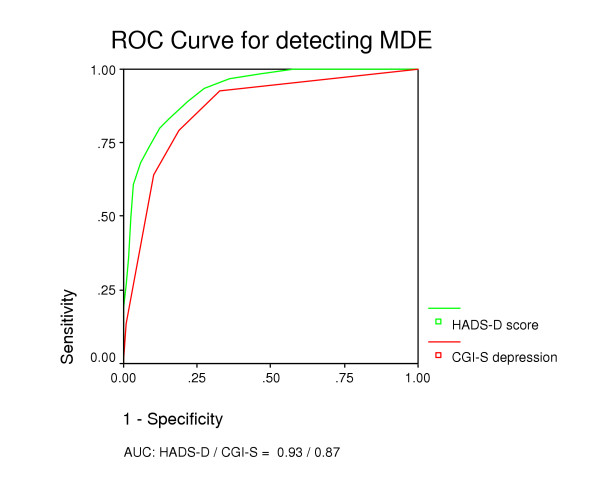
Results: The HADS-A had optimal cut off > or =8 (sensitivity 0.89, specificity 0.75), AUC 0.88 and 76% of patients were correctly classified in relation to GAD. The HADS-D had by optimal cut off > or =8 (sensitivity 0.80 and specificity 0.88) AUC 0.93 and 87% of the patients were correctly classified in relation to MDE. Proportions of the total correctly classified at the CGI-S optimal cut-off > or =3 were 83% of patients for GAD and 81% for MDE.
Conclusion: The results indicate that addition of the patients' HADS scores to GPs' information could improve their diagnostic accuracy of GAD and MDE.
Figures
References
-
- Üstün TB, Sartorius N. Mental illness in general health care. Chichester: Wiley; 1995.
-
- Goldberg D, Steele JJ, Johnsen A, Smith C. Ability of primary care physicians to make accurate ratings of psychiatric symptoms. Arch Gen Psychiatry. 1982;39:829–33. - PubMed
-
- Feinstein RE, Brewer AA, Editors . Primary care psychiatry and behavioral medicine. New York: Springer; 1999.
-
- Munk-Jørgensen P, Fink P, Brevik JI, Dalgard OS, Engberg M, Hansson L, Holm M, Joukamaa M, Karlsson H, Lehtinen V, Nettbladt P, Stefansson C, Sørensem L, Jensen J, Borgquist L, Sandanger I, Nordström G. Psychiatric morbidity inn primary public health care: a multicentre investigation. Part II. Hidden morbidity and choice of treatment. Acta Psychiatr Scand. 1997;95:6–12. - PubMed
