

Prospective phase 1/2 study of rituximab in childhood and adolescent chronic immune thrombocytopenic purpura
- PMID: 16352811
- PMCID: PMC1895391
- DOI: 10.1182/blood-2005-08-3518
Prospective phase 1/2 study of rituximab in childhood and adolescent chronic immune thrombocytopenic purpura
Abstract
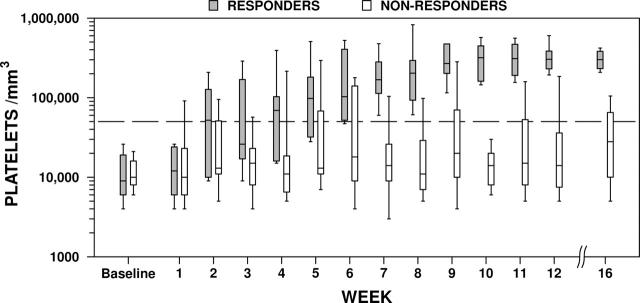
We assessed safety and efficacy of rituximab in a prospective study of 36 patients, age 2.6 to 18.3 years, with severe chronic immune thrombocytopenic purpura (ITP). The primary outcome of sustained platelets above 50 x 10(9)/L (50,000/mm3) during 4 consecutive weeks, starting in weeks 9 to 12, was achieved by 11 of 36 patients (31%, confidence interval [CI], 16% to 48%). Median response time was 1 week (range, 1 to 7 weeks). Attainment of the primary outcome was not associated with age, prior pharmacologic responses, prior splenectomy, ITP duration, screening platelet count, refractoriness, or IgM reduction. First-dose, infusion-related toxicity was common (47%) despite premedication. Significant drug-related toxicities included third-dose hypotension (n = 1) and serum sickness (n = 2). Peripheral B cells were depleted in all subjects. IgM decreased 3.4% per week, but IgG did not significantly decrease. Rituximab was well tolerated, with manageable infusion-related side effects, but 6% of subjects developed serum sickness. Rituximab is beneficial for some pediatric patients with severe, chronic ITP.
Figures
References
-
- Bennett CM, Bussel JB, Mahoney DH, Olson TA, Neufeld EJ. Prospective phase I/II study of rituximab in childhood chronic ITP (cITP) [abstract]. Pediatr Blood Cancer. 2005;55: 566.
-
- Kuhne T, Buchanan GR, Zimmerman S, et al. A prospective comparative study of 2540 infants and children with newly diagnosed idiopathic thrombocytopenic purpura (ITP) from the Intercontinental Childhood ITP Study Group. J Pediatr. 2003;143: 605-608. - PubMed
-
- Maloney D, Liles T, Czerwinski D, et al. Phase I clinical trial using escalating single-dose infusion of chimeric anti-CD20 monoclonal antibody (IDEC-C2B8) in patients with recurrent B-cell lymphoma. Blood. 1994;84: 2457-2466. - PubMed
-
- Maloney DG, Grillo-Lopez AJ, White CA, et al. IDEC-C2B8 (rituximab) anti-CD20 monoclonal antibody therapy in patients with relapsed low-grade non-Hodgkin's lymphoma. Blood. 1997;90: 2188-2195. - PubMed
-
- McLaughlin P, Grillo-Lopez AJ, Link BK, et al. Rituximab chimeric anti-CD20 monoclonal antibody therapy for relapsed indolent lymphoma: half of patients respond to a four-dose treatment program. J Clin Oncol. 1998;16: 2825-2833. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
