

Control of hyperuricemia in subjects with refractory gout, and induction of antibody against poly(ethylene glycol) (PEG), in a phase I trial of subcutaneous PEGylated urate oxidase
- PMID: 16356199
- PMCID: PMC1526556
- DOI: 10.1186/ar1861
Control of hyperuricemia in subjects with refractory gout, and induction of antibody against poly(ethylene glycol) (PEG), in a phase I trial of subcutaneous PEGylated urate oxidase
Abstract
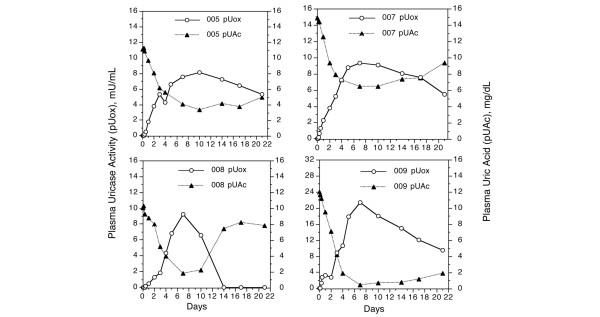
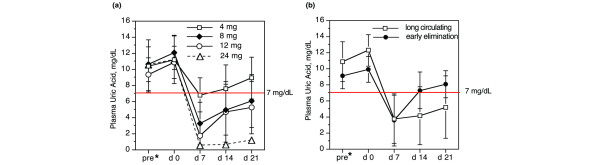
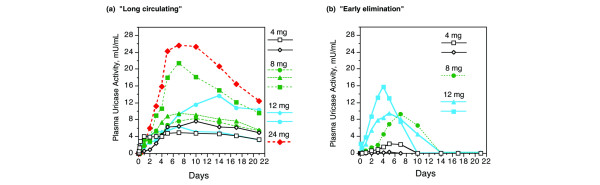
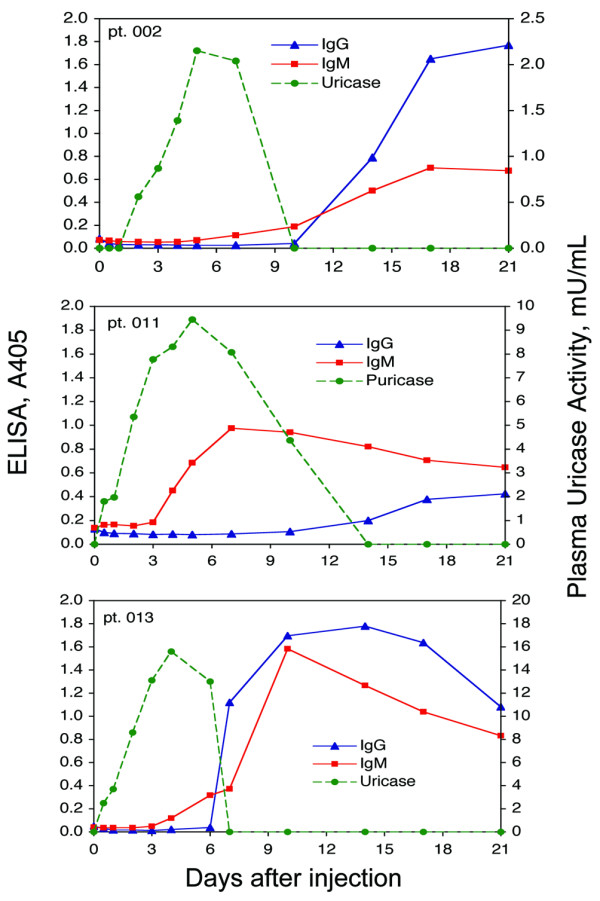
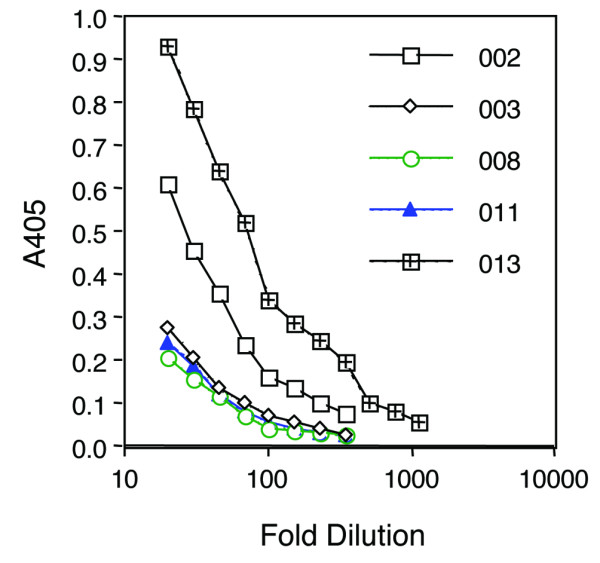
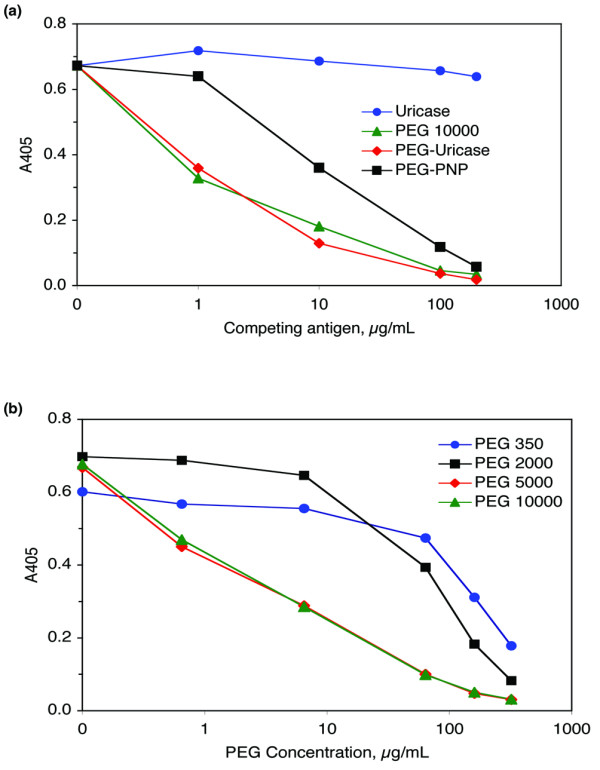
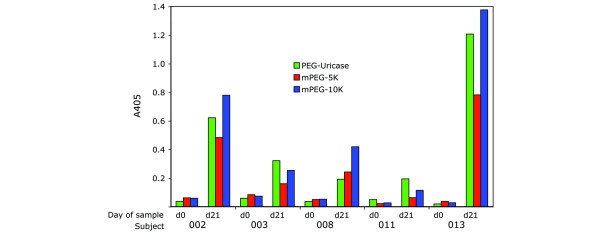
PEG-modified recombinant mammalian urate oxidase (PEG-uricase) is being developed as a treatment for patients with chronic gout who are intolerant of, or refractory to, available therapy for controlling hyperuricemia. In an open-label phase I trial, single subcutaneous injections of PEG-uricase (4 to 24 mg) were administered to 13 such subjects (11 had tophaceous gout), whose plasma uric acid concentration (pUAc) was 11.3 +/- 2.1 mg/dl (mean +/- SD). By day seven after injection of PEG-uricase, pUAc had declined by an average of 7.9 mg/dl and had normalized in 11 subjects, whose mean pUAc decreased to 2.8 +/- 2.2 mg/dl. At doses of 8, 12, and 24 mg, the mean pUAc at 21 days after injection remained no more than 6 mg/dl. In eight subjects, plasma uricase activity was still measurable at 21 days after injection (half-life 10.5 to 19.9 days). In the other five subjects, plasma uricase activity could not be detected beyond ten days after injection; this was associated with the appearance of relatively low-titer IgM and IgG antibodies against PEG-uricase. Unexpectedly, these antibodies were directed against PEG itself rather than the uricase protein. Three PEG antibody-positive subjects had injection-site reactions at 8 to 9 days after injection. Gout flares in six subjects were the only other significant adverse reactions, and PEG-uricase was otherwise well tolerated. A prolonged circulating life and the ability to normalize plasma uric acid in markedly hyperuricemic subjects suggest that PEG-uricase could be effective in depleting expanded tissue stores of uric acid in subjects with chronic or tophaceous gout. The development of anti-PEG antibodies, which may limit efficacy in some patients, is contrary to the general assumption that PEG is non-immunogenic. PEG immunogenicity deserves further investigation, because it has potential implications for other PEGylated therapeutic agents in clinical use.
Figures
References
-
- Becker MA. Hyperuricemia and gout. In: Scriver CR, Beaudet AL, Sly WS, Valle D, editor. The Metabolic and Molecular Bases of Inherited Disease. 8. New York: McGraw-Hill; 2001. pp. 2513–2535.
-
- Wortmann RL, Kelley WN. Gout and hyperuricemia. In: Ruddy S, Harris ED Jr, Sledge CB, editor. Kelley's Textbook of Rheumatology. 6. St Louis: WB Saunders; 2001. pp. 1339–1371.
-
- Riedel AA, Nelson M, Joseph-Ridge N, Wallace K, MacDonald P, Becker M. Compliance with allopurinol therapy among managed care enrollees with gout: a retrospective analysis of administrative claims. J Rheumatol. 2004;31:1575–1581. - PubMed
-
- London M, Hudson PM. Uricolytic activity of purified uricase in two human beings. Science. 1957;125:937–938. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
