

Evaluating mortality in intensive care units: contribution of competing risks analyses
- PMID: 16356211
- PMCID: PMC1550827
- DOI: 10.1186/cc3921
Evaluating mortality in intensive care units: contribution of competing risks analyses
Abstract
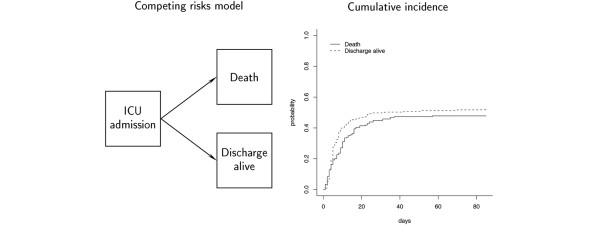
Introduction: Kaplan-Meier curves and logistic models are widely used to describe and explain the variability of survival in intensive care unit (ICU) patients. The Kaplan-Meier approach considers that patients discharged alive from hospital are 'non-informatively' censored (for instance, representative of all other individuals who have survived to that time but are still in hospital); this is probably wrong. Logistic models are adapted to this so-called 'competing risks' setting but fail to take into account censoring and differences in exposure time. To address these issues, we exemplified the usefulness of standard competing risks methods; namely, cumulative incidence function (CIF) curves and the Fine and Gray model.
Methods: We studied 203 mechanically ventilated cancer patients with acute respiratory failure consecutively admitted over a five-year period to a teaching hospital medical ICU. Among these patients, 97 died before hospital discharge. After estimating the CIF of hospital death, we used Fine and Gray models and logistic models to explain variability hospital mortality.
Results: The CIF of hospital death was 35.5% on day 14 and was 47.8% on day 60 (97/203); there were no further deaths. Univariate models, either the Fine and Gray model or the logistic model, selected the same eight variables as carrying independent information on hospital mortality at the 5% level. Results of multivariate were close, with four variables selected by both models: autologous stem cell transplantation, absence of congestive heart failure, neurological impairment, and acute respiratory distress syndrome. Two additional variables, clinically documented pneumonia and the logistic organ dysfunction, were selected by the Fine and Gray model.
Conclusion: The Fine and Gray model appears of interest when predicting mortality in ICU patients. It is closely related to the logistic model, through direct modeling of times to death, and can be easily extended to model non-fatal outcomes.
Figures
Comment in
-
Survival methods, including those using competing risk analysis, are not appropriate for intensive care unit outcome studies.Crit Care. 2006 Feb;10(1):103. doi: 10.1186/cc3949. Crit Care. 2006. PMID: 16420653 Free PMC article.
References
-
- Azoulay E, Alberti C, Bornstain C, Leleu G, Moreau D, Recher C, Chevret S, Le Gall JR, Brochard L, Schlemmer B. Improved survival in cancer patients requiring mechanical ventilatory support: impact of noninvasive mechanical ventilatory support. Crit Care Med. 2001;29:519–525. doi: 10.1097/00003246-200103000-00009. - DOI - PubMed
-
- de Irala-Estevez J, Martinez-Concha D, Diaz-Molina C, Masa-Calles J, Serrano del Castillo A, Fernandez-Crehuet Navajas R. Comparison of different methodological approaches to identify risk factors of nosocomial infection in intensive care units. Intensive Care Med. 2001;27:1254–1262. doi: 10.1007/s001340101007. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
