

Meta-analysis of hemodynamic optimization: relationship to methodological quality
- PMID: 16356226
- PMCID: PMC1414050
- DOI: 10.1186/cc3902
Meta-analysis of hemodynamic optimization: relationship to methodological quality
Abstract
Introduction: To review systematically the effect of interventions aimed at hemodynamic optimization and to relate this to the quality of individual published trials.
Methods: A systematic, computerized bibliographic search of published studies and citation reviews of relevant studies was performed. All randomized clinical trials in which adult patients were included in a trial deliberately aiming at an optimized or maximized hemodynamic condition of the patients (with oxygen delivery, cardiac index, oxygen consumption, mixed venous oxygen saturation and/or stroke volume as end-points) were selected. A total of 30 studies were selected for independent review. Two reviewers extracted data on population, intervention, outcome and methodological quality. Agreement between reviewers was high: differences were eventually resolved by third-party decision. The methodological quality of the studies was moderate (mean 9.0, SD 1.7), and the outcomes of the randomized clinical trials were not related to their quality.
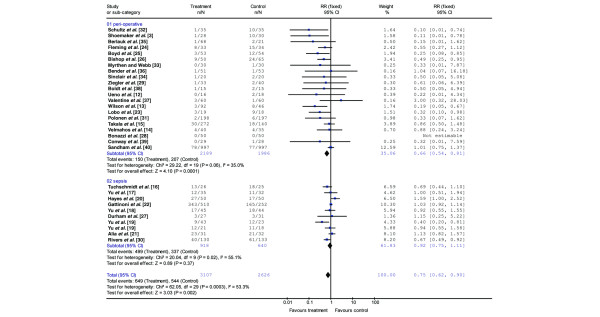
Results: Efforts to achieve an optimized hemodynamic condition resulted in a decreased mortality rate (relative risk ratio (RR) 0.75 (95% confidence interval (CI) 0.62 to 0.90) in all studies combined. This was due to a significantly decreased mortality in peri-operative intervention studies (RR 0.66 (95% CI 0.54 to 0.81). Overall, patients with sepsis and overt organ failure do not benefit from this method (RR 0.92 (95% CI 0.75 to 1.11)).
Conclusion: This systematic review showed that interventions aimed at hemodynamic optimization reduced mortality. In particular, trials including peri-operative interventions aimed at the hemodynamic optimization of high-risk surgical patients reduce mortality. Overall, this effect was not related to the trial quality.
Figures
References
-
- Wo CC, Shoemaker WC, Appel PL, Bishop MH, Kram HB, Hardin E. Unreliability of blood pressure and heart rate to evaluate cardiac output in emergency resuscitation and critical illness. Crit Care Med. 1993;21:218–223. - PubMed
-
- Bishop MH, Shoemaker WC, Appel PL, Wo CJ, Zwick C, Kram HB, Meade P, Kennedy F, Fleming AW. Relationship between supranormal circulatory values, time delays, and outcome in severely traumatized patients. Crit Care Med. 1993;21:56–63. - PubMed
-
- Shoemaker WC, Appel PL, Kram HB, Waxman K, Lee TS. Prospective trial of supranormal values of survivors as therapeutic goals in high-risk surgical patients. Chest. 1988;94:1176–1186. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
