

Spontaneous breathing with airway pressure release ventilation favors ventilation in dependent lung regions and counters cyclic alveolar collapse in oleic-acid-induced lung injury: a randomized controlled computed tomography trial
- PMID: 16356227
- PMCID: PMC1414014
- DOI: 10.1186/cc3908
Spontaneous breathing with airway pressure release ventilation favors ventilation in dependent lung regions and counters cyclic alveolar collapse in oleic-acid-induced lung injury: a randomized controlled computed tomography trial
Abstract
Introduction: Experimental and clinical studies have shown a reduction in intrapulmonary shunt with spontaneous breathing during airway pressure release ventilation (APRV) in acute lung injury. This reduction was related to reduced atelectasis and increased aeration. We hypothesized that spontaneous breathing will result in better ventilation and aeration of dependent lung areas and in less cyclic collapse during the tidal breath.
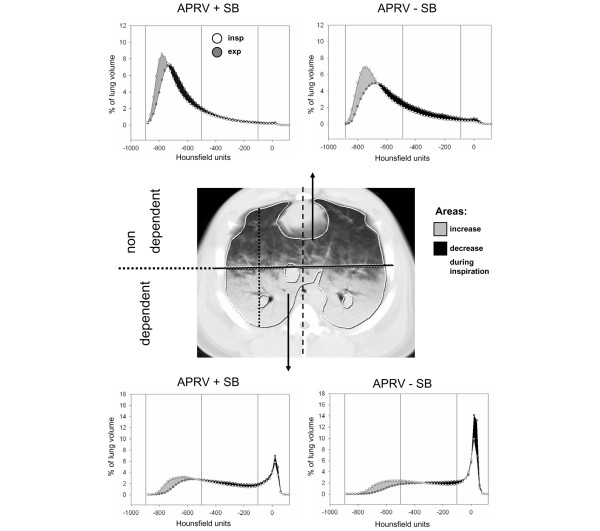
Methods: In this randomized controlled experimental trial, 22 pigs with oleic-acid-induced lung injury were randomly assigned to receive APRV with or without spontaneous breathing at comparable airway pressures. Four hours after randomization, dynamic computed tomography scans of the lung were obtained in an apical slice and in a juxtadiaphragmatic transverse slice. Analyses of regional attenuation were performed separately in nondependent and dependent halves of the lungs on end-expiratory scans and end-inspiratory scans. Tidal changes were assessed as differences between inspiration and expiration of the mechanical breaths.
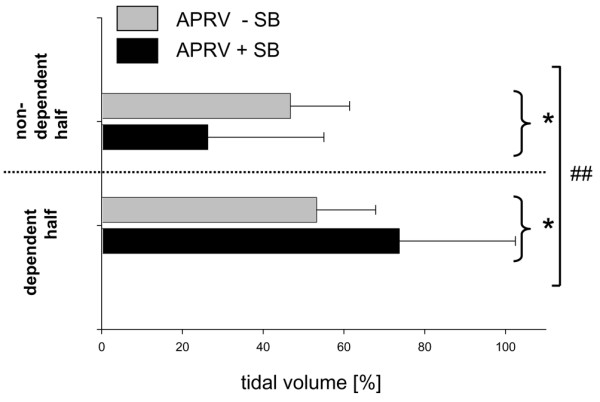
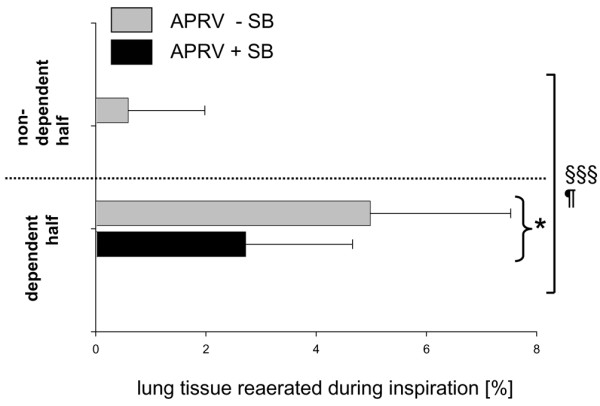
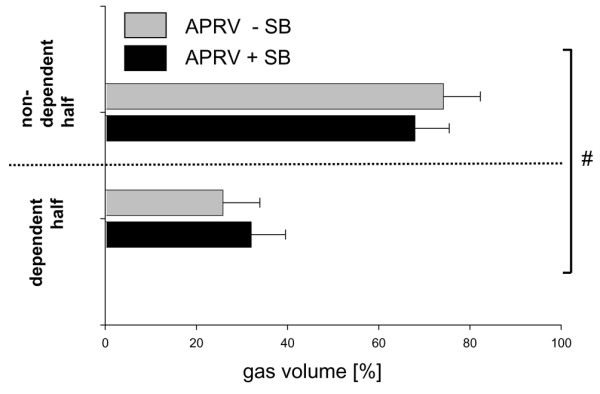
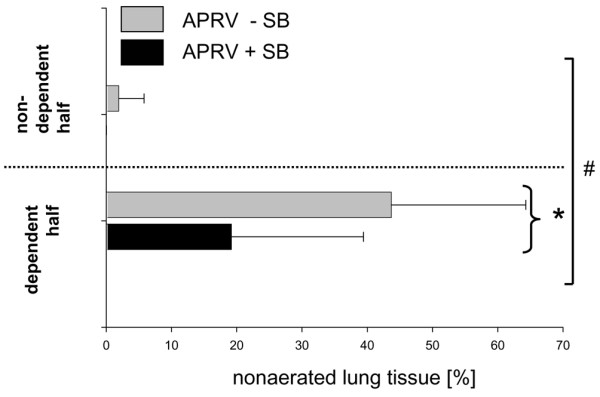
Results: Whereas no differences were observed in the apical slices, spontaneous breathing resulted in improved tidal ventilation of dependent lung regions (P < 0.05) and less cyclic collapse (P < 0.05) in the juxtadiaphragmatic slices. In addition, with spontaneous breathing, the end-expiratory aeration increased and nonaerated tissue decreased in dependent lung regions close to the diaphragm (P < 0.05 for the interaction ventilator mode and lung region).
Conclusion: Spontaneous breathing during APRV redistributes ventilation and aeration to dependent, usually well-perfused, lung regions close to the diaphragm, and may thereby contribute to improved arterial oxygenation. Spontaneous breathing also counters cyclic collapse, which is a risk factor for ventilation-associated lung injury.
Figures
Comment in
-
Assisted spontaneous breathing during early acute lung injury.Crit Care. 2006 Feb;10(1):102. doi: 10.1186/cc3953. Crit Care. 2006. PMID: 16420654 Free PMC article.
References
-
- Downs JB, Stock MC. Airway pressure release ventilation: a new concept in ventilatory support. Crit Care Med. 1987;15:459–461. - PubMed
-
- Stock MC, Downs JB, Froclicher DA. Airway pressure release ventilation. Crit Care Med. 1987;15:462–466. - PubMed
-
- Baum M, Benzer H, Putensen C, Koller W, Putz G. [Biphasic positive airway pressure (BIPAP) – a new form of augmented ventilation] Anaesthesist. 1989;38:452–458. - PubMed
-
- Putensen C, Zech S, Wrigge H, Zinserling J, Stuber F, von Spiegel T, Mutz N. Long-term effects of spontaneous breathing during ventilatory support in patients with acute lung injury. Am J Respir Crit Care Med. 2001;164:43–49. - PubMed
-
- Sydow M, Burchardi H, Ephraim E, Zielmann S, Crozier TA. Long-term effects of two different ventilatory modes on oxygenation in acute lung injury. Comparison of airway pressure release ventilation and volume-controlled inverse ratio ventilation. Am J Respir Crit Care Med. 1994;149:1550–1556. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
