

Clinical review: Positive end-expiratory pressure and cardiac output
- PMID: 16356246
- PMCID: PMC1414045
- DOI: 10.1186/cc3877
Clinical review: Positive end-expiratory pressure and cardiac output
Abstract
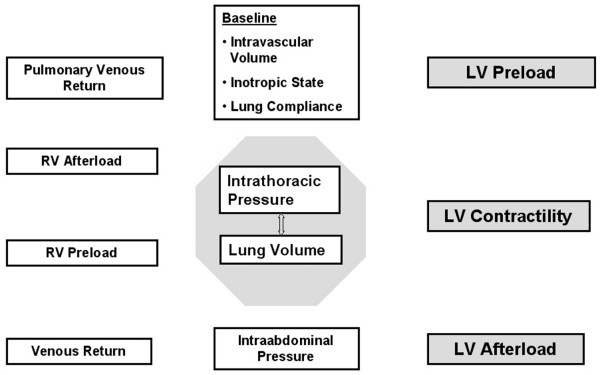
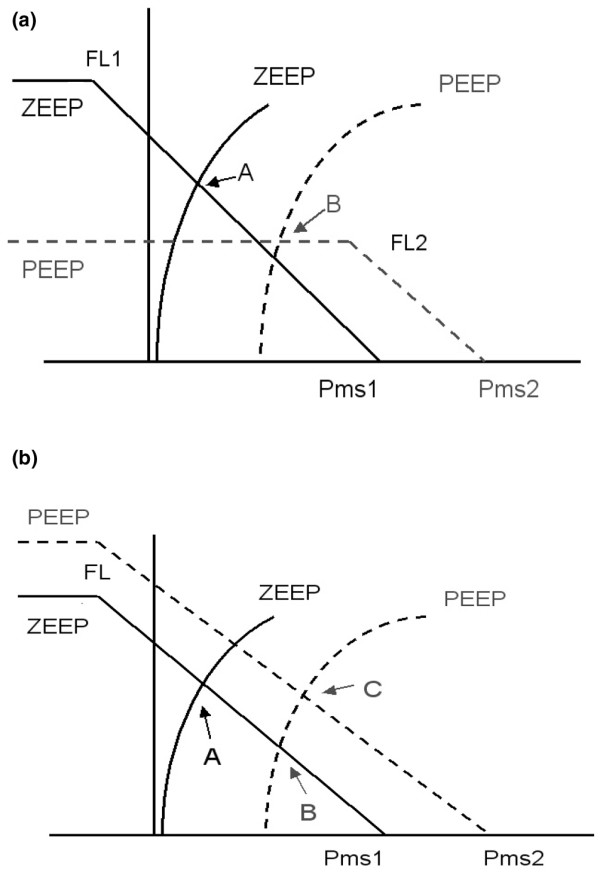
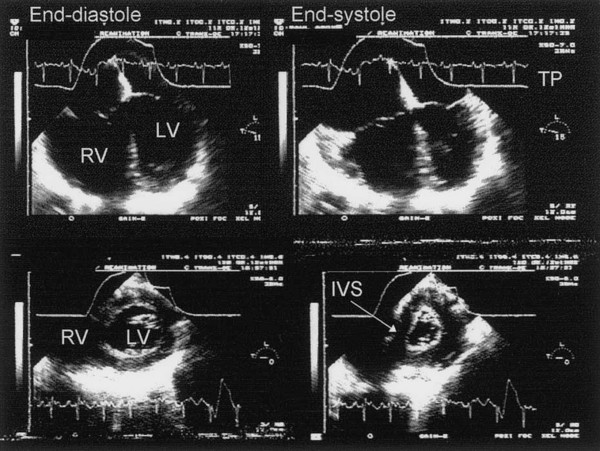
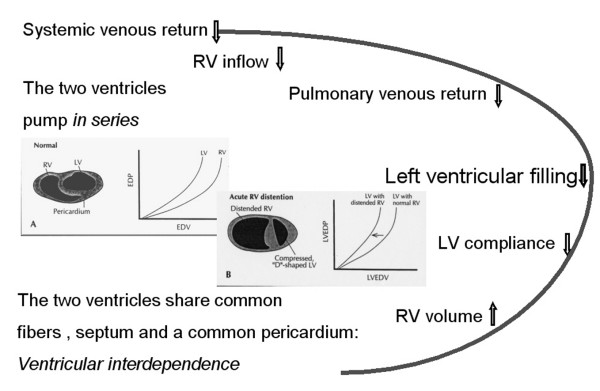
In patients with acute lung injury, high levels of positive end-expiratory pressure (PEEP) may be necessary to maintain or restore oxygenation, despite the fact that 'aggressive' mechanical ventilation can markedly affect cardiac function in a complex and often unpredictable fashion. As heart rate usually does not change with PEEP, the entire fall in cardiac output is a consequence of a reduction in left ventricular stroke volume (SV). PEEP-induced changes in cardiac output are analyzed, therefore, in terms of changes in SV and its determinants (preload, afterload, contractility and ventricular compliance). Mechanical ventilation with PEEP, like any other active or passive ventilatory maneuver, primarily affects cardiac function by changing lung volume and intrathoracic pressure. In order to describe the direct cardiocirculatory consequences of respiratory failure necessitating mechanical ventilation and PEEP, this review will focus on the effects of changes in lung volume, factors controlling venous return, the diastolic interactions between the ventricles and the effects of intrathoracic pressure on cardiac function, specifically left ventricular function. Finally, the hemodynamic consequences of PEEP in patients with heart failure, chronic obstructive pulmonary disease and acute respiratory distress syndrome are discussed.
Figures
References
-
- Dreyfuss D, Saumon G. Ventilator-induced lung injury. Lessons from experimental studies. Am J Respir Crit Care Med. 1998;157:294–330. - PubMed
-
- Maggiore SM, Jonson B, Richard JC, Jaber S, Lemaire F, Brochard L. Alveolar derecruitment at decremental positive end-expiratory pressure levels in acute lung injury: comparison with the lower inflection point, oxygenation, and compliance. Am J Respir Crit Care Med. 2001;164:795–801. - PubMed
-
- Rouby JJ, Lu Q, Goldstein I. Selecting the right level of positive end-expiratory pressure in patients with acute respiratory distress syndrome. Am J Respir Crit Care Med. 2002;165:1182–1186. - PubMed
-
- Cournand A, Motley HL, Werko L, Richards D. Physiological studies of the effects of intermittent positive pressure breathing on cardiac output in man. Am J Physiol. 1948;152:162–174. - PubMed
-
- Viquerat CE, Righetti A, Suter PM. Biventricular volumes and function in patients with adult respiratory distress syndrome ventilated with PEEP. Chest. 1983;83:509–514. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
