

Effects of human cerebellar thalamus disruption on adaptive control of reaching
- PMID: 16357337
- PMCID: PMC1560096
- DOI: 10.1093/cercor/bhj087
Effects of human cerebellar thalamus disruption on adaptive control of reaching
Abstract
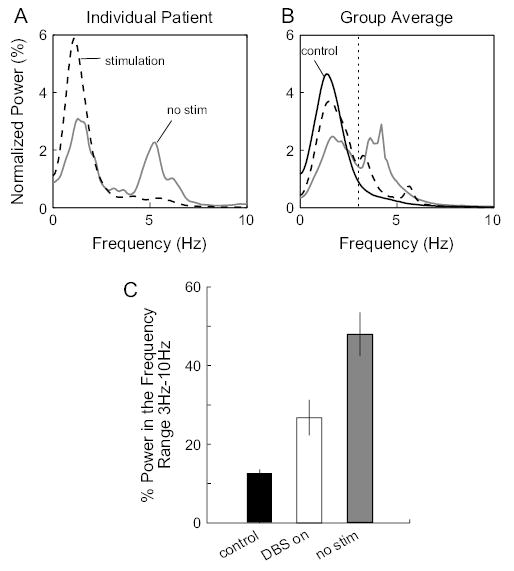
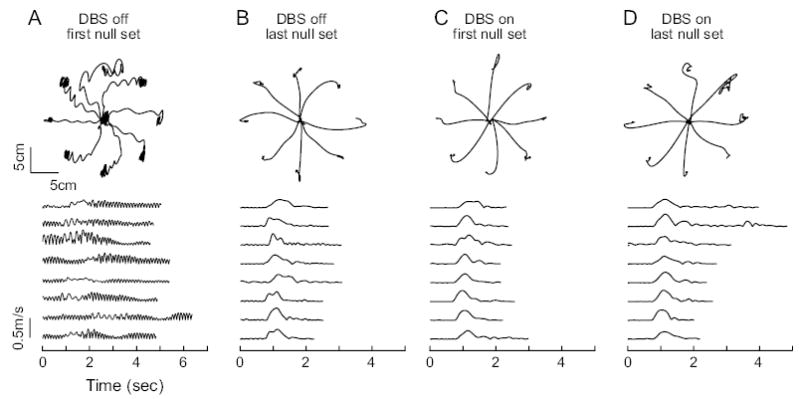
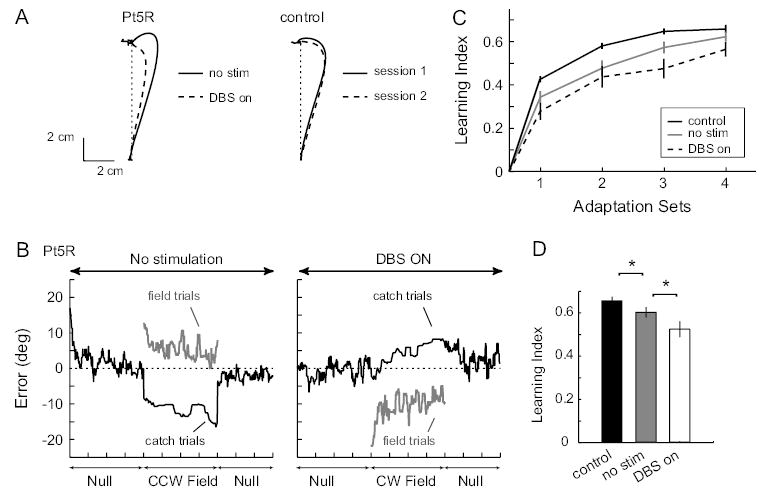
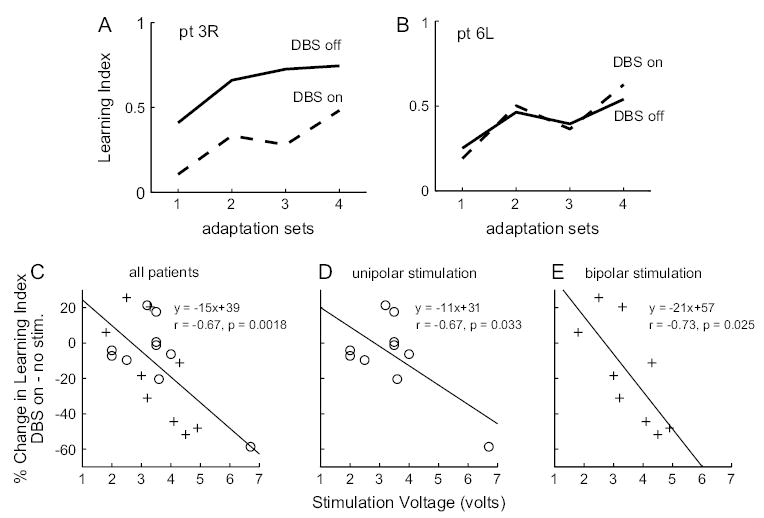
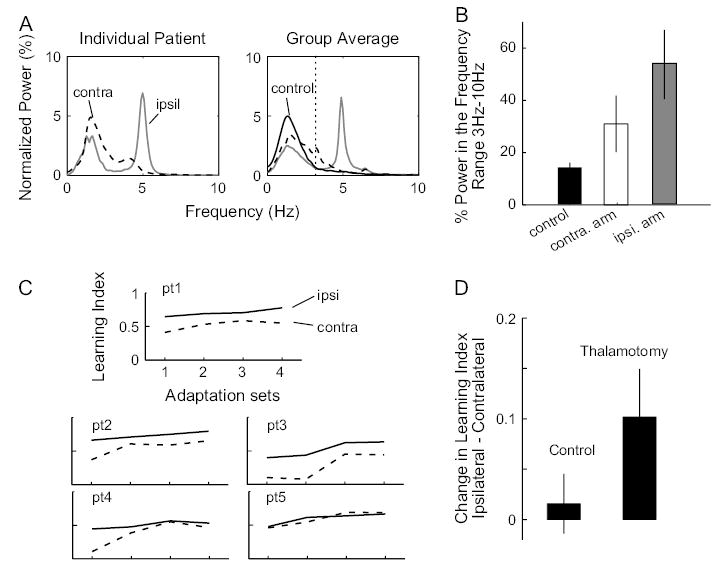
Lesion or degeneration of the cerebellum can profoundly impair adaptive control of reaching in humans. Computational models have proposed that internal models that help control movements form in the cerebellum and influence planned motor output through the cerebello-thalamo-cortical pathway. However, lesion studies of the cerebellar thalamus have not consistently found impairment in reaching or adaptation of reaching. To elucidate the role of the cerebellar thalamus in humans, we studied a group of essential tremor (ET) patients with deep brain stimulation (DBS) electrodes placed in the cerebellar thalamus. The stimulation can be turned on or off remotely and is thought to reduce tremor by blocking the spread of the pathological output from the cerebellum. We studied the effect of thalamic DBS on the ability to adapt arm movements to novel force fields. Although thalamic DBS resulted in a dramatic and significant reduction of tremor in ET, it also impaired motor adaptation: the larger the stimulation voltage, the greater the reduction in rates of adaptation. We next examined ET patients that had undergone unilateral thalamotomy in the cerebellar thalamus and found that adaptation with the contralateral arm was impaired compared with the ipsilateral arm. Therefore, although both lesion and electrical stimulation of the cerebellar thalamus are highly effective in reducing tremor, they significantly impair the ability of the brain to form internal models of action. Adaptive control of reaching appears to depend on the integrity of the cerebello-thalamo-cortical pathway.
Figures
References
-
- Anderson ME, Postupna N, Ruffo M. Effects of high-frequency stimulation in the internal globus pallidus on the activity of thalamic neurons in the awake monkey. J Neurophysiol. 2003;89:1150–1160. - PubMed
-
- Bastian AJ, Martin TA, Keating JG, Thach WT. Cerebellar ataxia: abnormal control of interaction torques across multiple joints. J Neurophysiol. 1996;76:492–509. - PubMed
-
- Ceballos-Baumann AO, Boecker H, Fogel W, Alesch F, Bartenstein P, Conrad B, Diederich N, von Falkenhayn I, Moringlane JR, Schwaiger M, Tronnier VM. Thalamic stimulation for essential tremor activates motor and deactivates vestibular cortex. Neurology. 2001;56:1347–1354. - PubMed
-
- Conrad B, Matsunami K, Meyer-Lohmann J, Wiesendanger M, Brooks VB. Cortical load compensation during voluntary elbow movements. Brain Res. 1974;71:507–514. - PubMed
-
- Deuschl G, Bergman H. Pathophysiology of nonparkinsonian tremors. Mov Disord. 2002;17(Suppl 3):S41–S48. - PubMed
