

Overriding of drug safety alerts in computerized physician order entry
- PMID: 16357358
- PMCID: PMC1447540
- DOI: 10.1197/jamia.M1809
Overriding of drug safety alerts in computerized physician order entry
Abstract
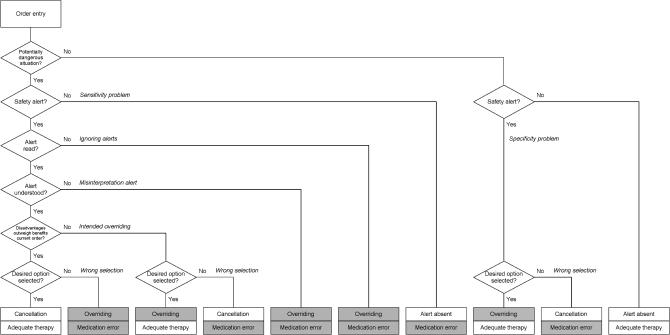
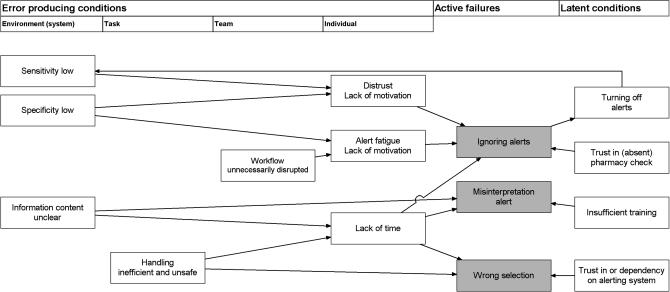
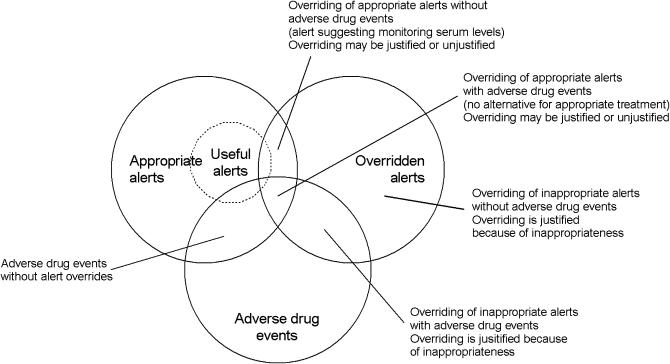
Many computerized physician order entry (CPOE) systems have integrated drug safety alerts. The authors reviewed the literature on physician response to drug safety alerts and interpreted the results using Reason's framework of accident causation. In total, 17 papers met the inclusion criteria. Drug safety alerts are overridden by clinicians in 49% to 96% of cases. Alert overriding may often be justified and adverse drug events due to overridden alerts are not always preventable. A distinction between appropriate and useful alerts should be made. The alerting system may contain error-producing conditions like low specificity, low sensitivity, unclear information content, unnecessary workflow disruptions, and unsafe and inefficient handling. These may result in active failures of the physician, like ignoring alerts, misinterpretation, and incorrect handling. Efforts to improve patient safety by increasing correct handling of drug safety alerts should focus on the error-producing conditions in software and organization. Studies on cognitive processes playing a role in overriding drug safety alerts are lacking.
Figures
References
-
- Kaushal R, Shojania KG, Bates DW. Effects of computerized physician order entry and clinical decision support systems on medication safety. A systematic review. Arch Intern Med. 2003;163:1409–16. - PubMed
-
- Glassman PA, Simon B, Belperio P, Lanto A. Improving recognition of drug interactions. Benefits and barriers to using automated drug alerts. Med Care. 2002;40:1161–71. - PubMed
-
- Raschke RA, Gollihare B, Wunderlich TA, Guidry JR, Leibowitz AI, Peirce JC, et al. A computer alert system to prevent injury from adverse drug events. JAMA. 1998;280:1317–20. - PubMed
-
- Hunt DL, Haynes RB, Hanna SE, Smith K. Effects of computer-based clinical decision support systems on physician performance an patient outcomes. JAMA. 1998;280:1339–46. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
