

Integrating "best of care" protocols into clinicians' workflow via care provider order entry: impact on quality-of-care indicators for acute myocardial infarction
- PMID: 16357360
- PMCID: PMC1447538
- DOI: 10.1197/jamia.M1656
Integrating "best of care" protocols into clinicians' workflow via care provider order entry: impact on quality-of-care indicators for acute myocardial infarction
Abstract
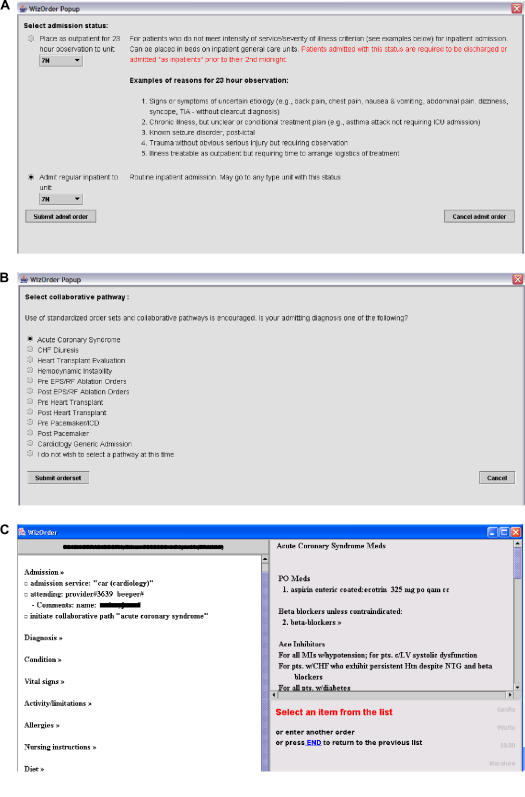
Objective: In the context of an inpatient care provider order entry (CPOE) system, to evaluate the impact of a decision support tool on integration of cardiology "best of care" order sets into clinicians' admission workflow, and on quality measures for the management of acute myocardial infarction (AMI) patients.
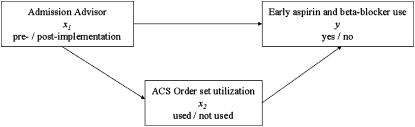
Design: A before-and-after study of physician orders evaluated (1) per-patient use rates of standardized acute coronary syndrome (ACS) order set and (2) patient-level compliance with two individual recommendations: early aspirin ordering and beta-blocker ordering.
Measurements: The effectiveness of the intervention was evaluated for (1) all patients with ACS (suspected for AMI at the time of admission) (N = 540) and (2) the subset of the ACS patients with confirmed discharge diagnosis of AMI (n = 180) who comprise the recommended target population who should receive aspirin and/or beta-blockers. Compliance rates for use of the ACS order set, aspirin ordering, and beta-blocker ordering were calculated as the percentages of patients who had each action performed within 24 hours of admission.
Results: For all ACS admissions, the decision support tool significantly increased use of the ACS order set (p = 0.009). Use of the ACS order set led, within the first 24 hours of hospitalization, to a significant increase in the number of patients who received aspirin (p = 0.001) and a nonsignificant increase in the number of patients who received beta-blockers (p = 0.07). Results for confirmed AMI cases demonstrated similar increases, but did not reach statistical significance.
Conclusion: The decision support tool increased optional use of the ACS order set, but room for additional improvement exists.
Figures
Similar articles
-
Embedded guideline information without patient specificity in a commercial emergency department computerized order-entry system.Acad Emerg Med. 2006 Apr;13(4):452-8. doi: 10.1197/j.aem.2005.09.015. Epub 2006 Mar 10. Acad Emerg Med. 2006. PMID: 16531590
-
Intervention to increase the proportion of acute myocardial infarction or coronary artery bypass graft patients receiving an order for aspirin at hospital discharge.J Manag Care Pharm. 2010 Jun;16(5):329-36. doi: 10.18553/jmcp.2010.16.5.329. J Manag Care Pharm. 2010. PMID: 20518585 Free PMC article.
-
Improved compliance with quality measures at hospital discharge with a computerized physician order entry system.Am Heart J. 2006 Mar;151(3):643-53. doi: 10.1016/j.ahj.2005.05.007. Am Heart J. 2006. PMID: 16504626
-
New recommendations from the 1999 American College of Cardiology/American Heart Association acute myocardial infarction guidelines.Ann Pharmacother. 2001 May;35(5):589-617. doi: 10.1345/aph.10319. Ann Pharmacother. 2001. PMID: 11346067 Review.
-
Antiplatelet intervention in acute coronary syndrome.Am J Ther. 2009 Sep-Oct;16(5):e29-40. doi: 10.1097/MJT.0b013e31804c7238. Am J Ther. 2009. PMID: 19092648 Review.
Cited by
-
CDS-Compare: A Web Application for Machine Learning Assisted Curation of Clinical Order Sets.Stud Health Technol Inform. 2022 May 25;294:465-469. doi: 10.3233/SHTI220502. Stud Health Technol Inform. 2022. PMID: 35612123 Free PMC article.
-
Use of order sets in inpatient computerized provider order entry systems: a comparative analysis of usage patterns at seven sites.Int J Med Inform. 2012 Nov;81(11):733-45. doi: 10.1016/j.ijmedinf.2012.04.003. Epub 2012 Jul 18. Int J Med Inform. 2012. PMID: 22819199 Free PMC article.
-
Order sets in computerized physician order entry systems: an analysis of seven sites.AMIA Annu Symp Proc. 2010 Nov 13;2010:892-6. AMIA Annu Symp Proc. 2010. PMID: 21347107 Free PMC article.
-
Extracting Actionable Recommendations for Modifying Enterprise Order Set Templates from CPOE Utilization Patterns.AMIA Annu Symp Proc. 2018 Apr 16;2017:950-958. eCollection 2017. AMIA Annu Symp Proc. 2018. PMID: 29854162 Free PMC article.
-
Viewpoint: controversies surrounding use of order sets for clinical decision support in computerized provider order entry.J Am Med Inform Assoc. 2007 Jan-Feb;14(1):41-7. doi: 10.1197/jamia.M2184. Epub 2006 Oct 26. J Am Med Inform Assoc. 2007. PMID: 17068352 Free PMC article.
References
-
- Park RE, Brook RH, Kosecoff J, et al. Explaining variations in hospital death rates. Randomness, severity of illness, quality of care. JAMA. 1990;264:484–90. - PubMed
-
- Institute of Medicine. Crossing the quality chasm: a new health system for the 21st century. Washington, DC: National Academy Press, 2001. - PubMed
-
- Critical pathways for management of patients with acute coronary syndromes: an assessment by the National Heart Attack Alert Program. Am Heart J. 2002;143:777–89. - PubMed
-
- Pearson SD, Goulart-Fisher D, Lee TH. Critical pathways as a strategy for improving care: problems and potential. Ann Intern Med. 1995;123:941–8. - PubMed
-
- Grimshaw JM, Russell IT. Effect of clinical guidelines on medical practice: a systematic review of rigorous evaluations. Lancet. 1993;342:1317–22. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
