

Liver metastases of colorectal cancer: US, CT or MR?
- PMID: 16361131
- PMCID: PMC1665297
- DOI: 10.1102/1470-7330.2005.0035
Liver metastases of colorectal cancer: US, CT or MR?
Abstract
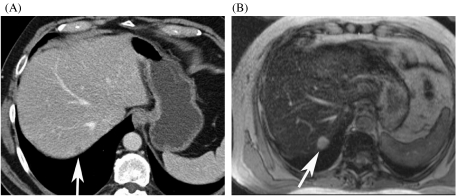
In contrast to other extrahepatic malignancies many colorectal cancers can be cured even when there is metastatic spread to the liver. The diagnosis of liver metastases relies totally on imaging to decide which patients may be surgical candidates. The diagnostic value of ultrasound with contrast agents, multidetector CT and MR imaging with non-specific gadolinium chelates and liver-specific contrast agent is discussed. Nowadays MDCT is the mainstay of staging and follow-up of these patients, because it provides good coverage of the liver and the complete abdomen and the chest in one session. MR imaging has been shown to be superior to helical CT in the preoperative assessment of colorectal liver metastases. Large studies are needed to define the role of MDCT vs. MRI staging in patients referred for resection of liver metastases.
International Cancer Imaging Society.
Figures

Similar articles
-
Detection of colo-rectal liver metastases: prospective comparison of contrast enhanced US, multidetector CT, PET/CT, and 1.5 Tesla MR with extracellular and reticulo-endothelial cell specific contrast agents.Abdom Imaging. 2010 Oct;35(5):511-21. doi: 10.1007/s00261-009-9555-2. Epub 2009 Jun 27. Abdom Imaging. 2010. PMID: 19562412
-
Real-time ultrasonography-computed tomography fusion imaging for staging of hepatic metastatic involvement in patients with colorectal cancer: initial results from comparison to US seeing separate CT images and to multidetector-row CT alone.Invest Radiol. 2010 Aug;45(8):491-501. doi: 10.1097/RLI.0b013e3181ddd3da. Invest Radiol. 2010. PMID: 20458251
-
[Liver metastases of colorectal cancers. Detection and delineation of their extension using imaging].Bull Acad Natl Med. 2003;187(5):825-33; discussion 834. Bull Acad Natl Med. 2003. PMID: 14979049 Review. French.
-
Liver metastases from colorectal cancer: imaging with superparamagnetic iron oxide (SPIO)-enhanced MR imaging, computed tomography and positron emission tomography.Abdom Imaging. 2007 Sep-Oct;32(5):624-34. doi: 10.1007/s00261-007-9297-y. Abdom Imaging. 2007. PMID: 17710359
-
Imaging modalities for the staging of patients with colorectal cancer.Neth J Med. 2012 Jan;70(1):26-34. Neth J Med. 2012. PMID: 22271811 Review.
Cited by
-
Impact of primary cancer features on behaviour of colorectal liver metastases and survival after hepatectomy.BJS Open. 2018 Sep 3;3(2):186-194. doi: 10.1002/bjs5.100. eCollection 2019 Apr. BJS Open. 2018. PMID: 30957066 Free PMC article.
-
Update on the role of imaging in management of metastatic colorectal cancer.Radiographics. 2014 Nov-Dec;34(7):1908-28. doi: 10.1148/rg.347130090. Radiographics. 2014. PMID: 25384292 Free PMC article. Review.
-
The Preoperative Assessment of Hepatic Tumours: Evaluation of UK Regional Multidisciplinary Team Performance.HPB Surg. 2013;2013:861681. doi: 10.1155/2013/861681. Epub 2013 Aug 22. HPB Surg. 2013. PMID: 24062601 Free PMC article.
-
A suggested guiding panel of seromarkers for efficient discrimination between primary and secondary human hepatocarcinoma.Tumour Biol. 2016 Feb;37(2):2539-46. doi: 10.1007/s13277-015-4025-7. Epub 2015 Sep 19. Tumour Biol. 2016. PMID: 26386723
-
Mathematical framework for activity-based cancer biomarkers.Proc Natl Acad Sci U S A. 2015 Oct 13;112(41):12627-32. doi: 10.1073/pnas.1506925112. Epub 2015 Sep 28. Proc Natl Acad Sci U S A. 2015. PMID: 26417077 Free PMC article.
References
-
- Rees M, John TG. Current status of surgery in colorectal metastases to the liver. Hepato-Gastroenterology. 2001;48:341–4. - PubMed
-
- Scheele J, Stangl R, Altendorf-Hofman A. Hepatic metastases from colorectal cancer: impact of surgical resection on the natural history. Br J Surg. 1990;77:1241–6. - PubMed
-
- Stangl R, Altendorf-Hofman A, Charnely R, Scheele J. Factors influencing the natural history of colorectal liver metastases. Lancet. 1994;343:1405–10. - PubMed
-
- von Herbay A, Vogt C, Willers R, Haussinger D. Real-time imaging with the sonographic contrast agent SonoVue: differentiation between benign and malignant hepatic lesions. J Ultrasound Med. 2004;23:1557–68. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical