

Review
doi: 10.1102/1470-7330.2005.0110.
Ultrasound of thyroid cancer
Affiliations
- PMID: 16361145
- PMCID: PMC1665239
- DOI: 10.1102/1470-7330.2005.0110
Item in Clipboard
Review
Ultrasound of thyroid cancer
Cancer Imaging.
.
Abstract
The management of thyroid nodules is multi-disciplinary and involves head and neck surgeons, pathologists and radiologists. Ultrasound is easy to perform, widely available, does not involve ionizing radiation and is readily combined with fine needle aspiration cytology (FNAC). It is therefore an ideal investigation of choice for evaluating thyroid nodules. It evaluates specific features that help in identifying the nature of the nodule and FNAC helps in diagnostic accuracy. In addition, following treatment for thyroid cancer ultrasound provides a safe tool for disease surveillance. This paper discusses the role of ultrasound in the management of patients with thyroid cancer.
International Cancer Imaging Society.
Figures
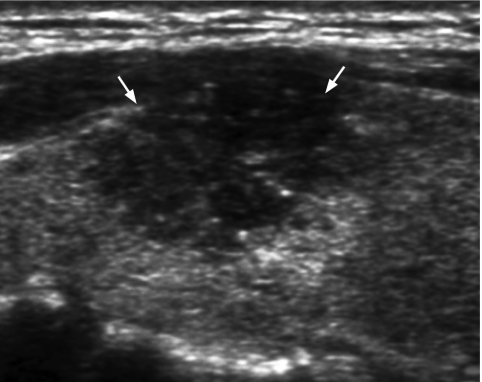
Longitudinal grey scale sonogram shows a solid, hypoechoic thyroid nodule (arrows) with ill-defined margins anteriorly. Histology: papillary carcinoma.
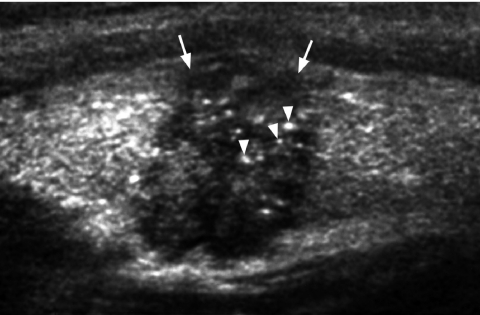
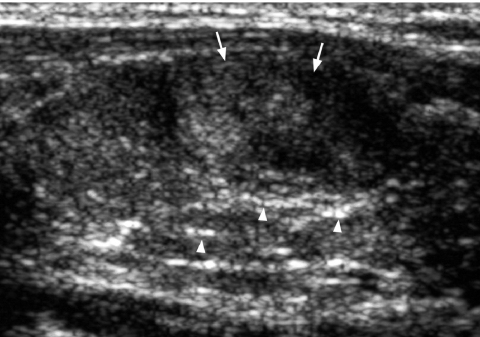
Longitudinal grey scale sonogram shows characteristic punctate calcification (arrowheads) within an ill-defined solid hypoechoic thyroid nodule (arrows) which is highly suggestive of papillary carcinoma.
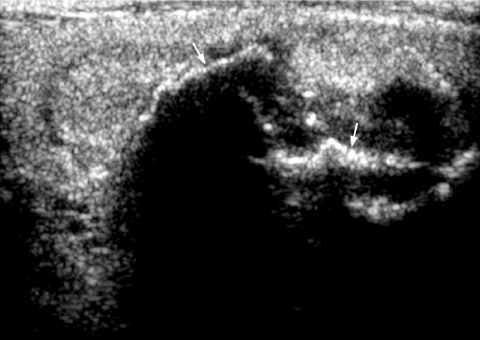
Longitudinal grey scale sonogram shows coarse calcifications (arrows) with dense shadowing within a thyroid nodule suggestive of benign calcification.
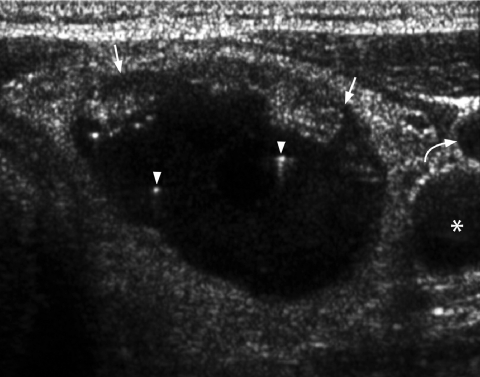
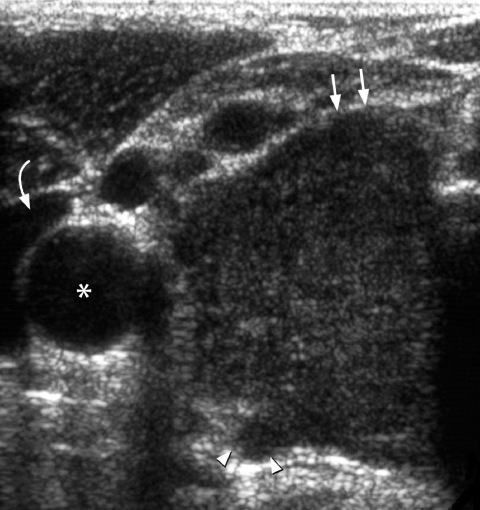
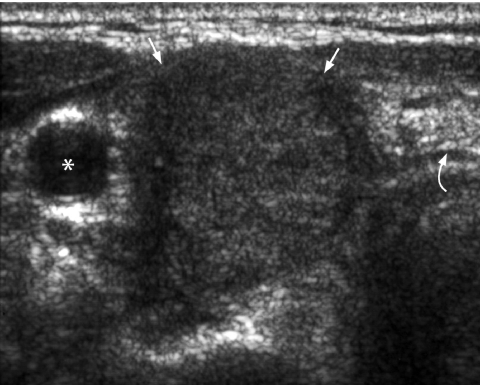
Transverse grey scale sonogram shows the presence of comet-tail artifacts (arrowheads) within a predominantly cystic thyroid nodule (arrows). Features are of a benign colloid nodule. Curved arrow identifies the internal jugular vein and asterisk marks the common carotid artery.

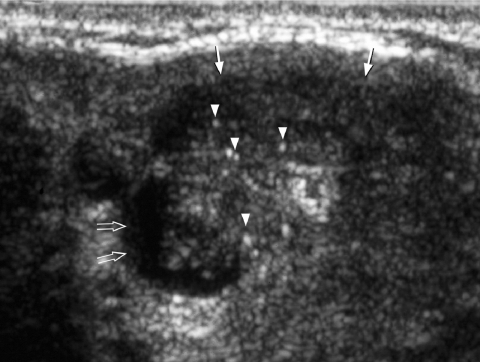
Longitudinal grey scale sonogram shows a well-defined heterogeneous thyroid nodule (arrows) with a large cystic component (arrowheads) and septation (open arrows). Features are compatible with a benign hyperplastic nodule.
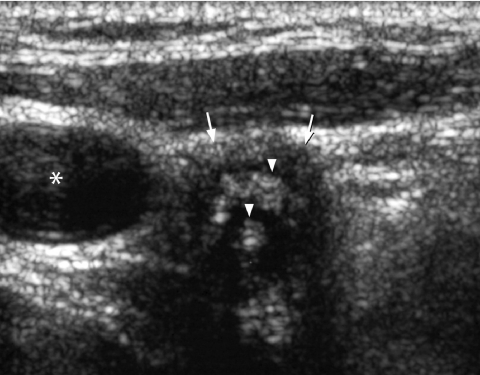
Transverse grey scale sonogram shows a cystic component (open arrows) within a papillary carcinoma (arrows) of the thyroid. The presence of punctate calcification (arrowheads) identifies its malignant nature.
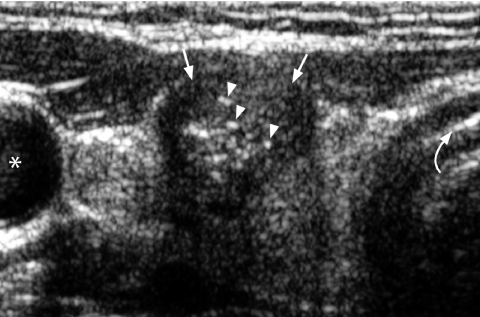
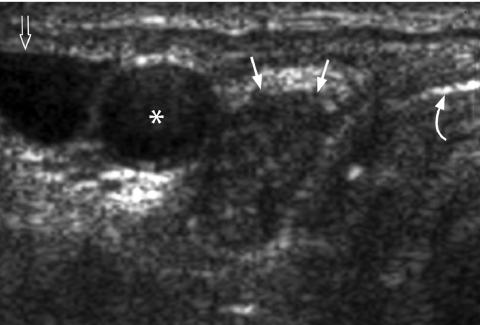
Transverse grey scale sonogram shows a solid, ill-defined, hypoechoic nodule (arrows) containing punctate calcification (arrowheads) in the right lobe of thyroid gland. Features are typical of papillary carcinoma of thyroid. Asterisk identifies the common carotid artery and curved arrow the trachea.
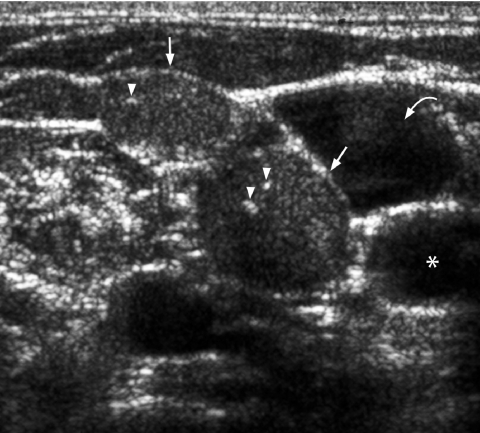
Transverse grey scale sonogram shows multiple round, solid, slightly hyperechoic cervical lymph nodes (arrows) with punctate calcification (arrowheads) in upper jugular chain. Features are suggestive of metastatic lymph nodes from primary papillary carcinoma of thyroid. Curved arrow identifies the internal jugular vein and asterisk marks the common carotid artery.
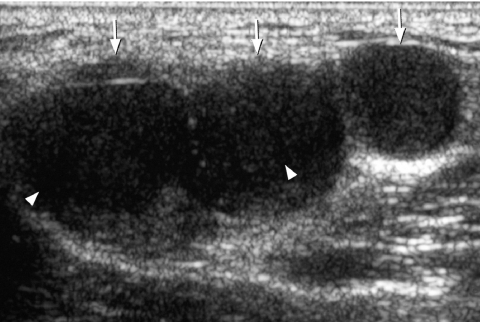
Transverse grey scale sonogram shows multiple enlarged hypoechoic cervical lymph nodes (arrows) with internal cystic necrosis (arrowheads) in a patient with metastatic lymphadenopathy from papillary carcinoma of thyroid.
Transverse grey scale sonogram shows a large, solid, hypoechoic mass (arrows) occupying the right lobe of thyroid gland. Note the presence of extra-thyroid spread posteriorly (arrowheads). Histology: anaplastic carcinoma. Curved arrow identifies the internal jugular vein and asterisk marks the common carotid artery.
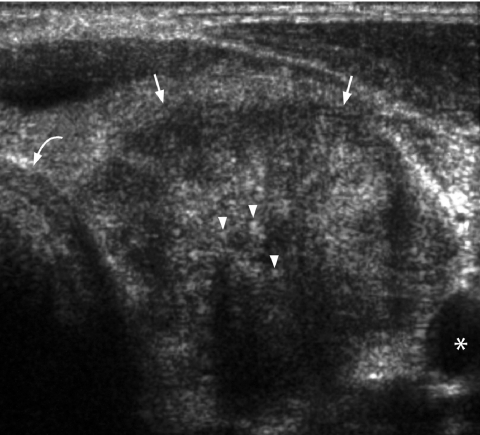
Transverse grey scale sonogram shows an ill-defined, solid, hypoechoic mass (arrows) occupying the left lobe of the thyroid gland. Multiple echogenic foci (arrowheads) casting dense posterior acoustic shadowing probably related to amyloid deposition and associated calcification. Appearance is that of a medullary carcinoma. Note how it closely resembles a papillary carcinoma. Curved arrow identifies the trachea and asterisk marks the common carotid artery.
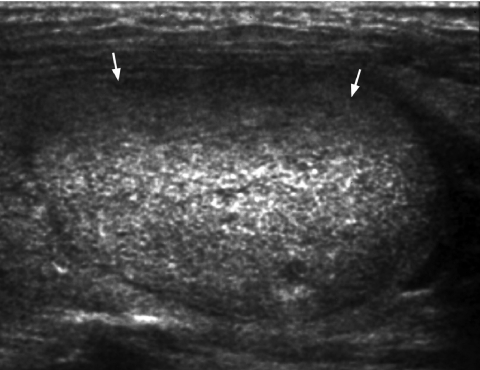
Longitudinal grey scale sonogram shows a well-defined hyperechoic nodule (arrows) in the left lobe of thyroid gland suggestive of a follicular lesion.
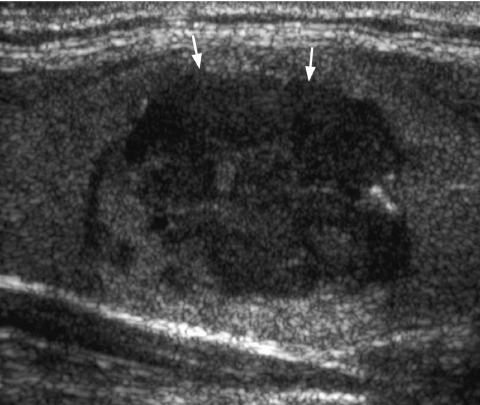
Longitudinal grey scale sonogram shows an ill-defined heterogeneous thyroid nodule (arrows). The hypoechoic nature of the follicular lesion raises the suspicion of follicular carcinoma which was confirmed on subsequent thyroidectomy.

Longitudinal grey scale sonogram shows the presence of floating hypoechoic thrombus (arrowheads) within the distended internal jugular vein (arrows). Colour/power Doppler will demonstrate vascularity in a tumour thrombus which distinguishes it from a stasis venous thrombus.
Transverse grey scale sonogram in a patient with known breast carcinoma shows a well-defined, solid, homogeneous hypoechoic mass (arrows) occupying the right lobe of thyroid. FNAC confirmed a metastatic carcinoma. The curved arrow identifies the trachea and the asterisk marks the common carotid artery.
Longitudinal grey scale sonogram shows an ill-defined, solid, hypoechoic nodule (arrows) in the thyroid gland. Thin echogenic lines (arrowheads) in the adjacent thyroid glandular parenchyma indicate background Hashimoto’s thyroiditis. Biopsy confirmed non-Hodgkin lymphoma of the thyroid gland.
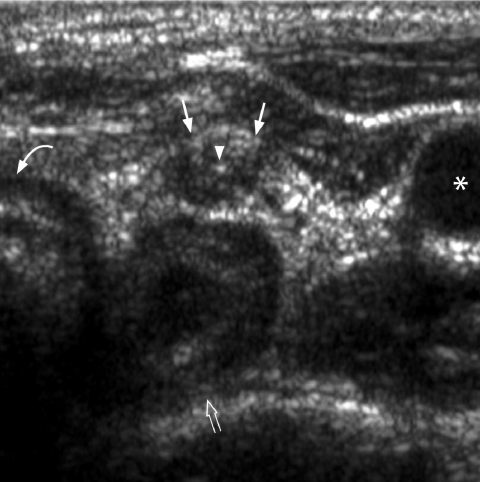
Transverse grey scale sonogram in a patient 1 year after total thyroidectomy for papillary carcinoma shows a small hypoechoic nodule (arrows) with punctate calcification (arrowhead) in the left thyroid bed. FNAC confirmed local tumour recurrence. The curved arrow identifies the trachea, the open arrow the oesophagus and the asterisk marks the common carotid artery.
Transverse grey scale sonogram shows an enlarged hypoechoic right paratracheal lymph node (arrows) 6-months after thyroidectomy for papillary carcinoma. Surgical excision confirmed regional nodal recurrence. The curved arrow identifies the trachea, the open arrow the internal jugular vein and the asterisk marks the common carotid artery.
Transverse grey scale sonogram shows an ill-defined hypoechoic nodule (arrows) in the right thyroid bed containing coarse echogenic foci (arrowheads). Features are suggestive of a suture granuloma. The asterisk identifies the common carotid artery.
Similar articles
-
The role of sonography in thyroid cancer.Radiol Clin North Am. 2014 Nov;52(6):1283-94. doi: 10.1016/j.rcl.2014.07.007. Epub 2014 Aug 29. Radiol Clin North Am. 2014. PMID: 25444106 Review.
-
Fine needle aspiration cytology in the management of solitary thyroid nodules--a comparison with other diagnostic modalities in cost-effectiveness.Singapore Med J. 1989 Dec;30(6):557-60. Singapore Med J. 1989. PMID: 2517548
-
Thyroid nodules: Α guide to assessment, treatment and follow-up.Maturitas. 2017 Feb;96:1-9. doi: 10.1016/j.maturitas.2016.11.002. Epub 2016 Nov 9. Maturitas. 2017. PMID: 28041586 Review.
-
Comparison of fine needle aspiration cytology, radioisotopic and ultrasound scanning in the management of thyroid nodules.Postgrad Med J. 1990 Nov;66(781):914-7. doi: 10.1136/pgmj.66.781.914. Postgrad Med J. 1990. PMID: 2176287 Free PMC article.
-
Diagnosis of thyroid metastasis in cancer patients with thyroid mass by fine needle aspiration cytology and ultrasonography.Zhonghua Yi Xue Za Zhi (Taipei). 2002 Mar;65(3):101-5. Zhonghua Yi Xue Za Zhi (Taipei). 2002. PMID: 12051452
Cited by
-
Thyroid hemiagenesis associated with Hurthle cell carcinoma: A case report.Int J Surg Case Rep. 2021 Sep;86:106372. doi: 10.1016/j.ijscr.2021.106372. Epub 2021 Sep 7. Int J Surg Case Rep. 2021. PMID: 34507192 Free PMC article.
-
"Nodule in Nodule" on Thyroid Ultrasonography: Possibility of Follicular Carcinoma Transformed from Benign Thyroid Tumor.Eur Thyroid J. 2017 Apr;6(2):101-107. doi: 10.1159/000452971. Epub 2016 Dec 13. Eur Thyroid J. 2017. PMID: 28589092 Free PMC article.
-
Re-Evaluation of 162 Malignant Thyroid Nodules that were Interpreted as Benign Based on Ultrasound Findings.Ultrasound Int Open. 2018 Oct;4(4):E110-E116. doi: 10.1055/a-0732-5795. Epub 2018 Oct 25. Ultrasound Int Open. 2018. PMID: 30370399 Free PMC article.
-
Imaging for staging and management of thyroid cancer.Cancer Imaging. 2008 Mar 25;8(1):57-69. doi: 10.1102/1470-7330.2008.0007. Cancer Imaging. 2008. PMID: 18390389 Free PMC article. Review.
-
The T4/T3 quotient as a risk factor for differentiated thyroid cancer: a case control study.J Otolaryngol Head Neck Surg. 2017 Apr 4;46(1):28. doi: 10.1186/s40463-017-0208-0. J Otolaryngol Head Neck Surg. 2017. PMID: 28376913 Free PMC article.
References
-
- Tunbridge WMG, Evered DC, Hall R, et al. The spectrum of thyroid disease in a community: the Whickham survey. Clin Endocrinol. 1977;7:481–93. - PubMed
-
- Vander JB, Gaston EA, Dawber TR. The significance of nontoxic thyroid nodules: final report of a 15-year study of the incidence of thyroid malignancy. Ann Intern Med. 1968;69:537–40. - PubMed
-
- Rojeski MT, Gharib H. Nodular thyroid disease: evaluation and management. N Engl J Med. 1985;313:428–36. - PubMed
-
- Rallison ML, Dobyns BM, Meikle AW, et al. Natural history of thyroid abnormalities: prevalence incidence, and regression of thyroid diseases in adolescent and young adults. Am J Med. 1991;91:363–70. - PubMed
-
- Lahey FH, Hare HF. Malignancy in adenomas of the thyroid. J Am Med Assoc. 1951;145:689–95. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical