

Imaging of lumps and bumps in the nose: a review of sinonasal tumours
- PMID: 16361146
- PMCID: PMC1665243
- DOI: 10.1102/1470-7330.2005.0111
Imaging of lumps and bumps in the nose: a review of sinonasal tumours
Abstract
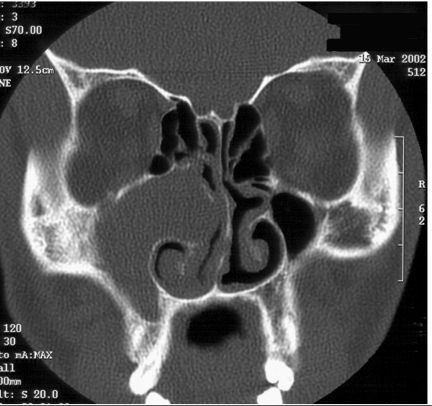
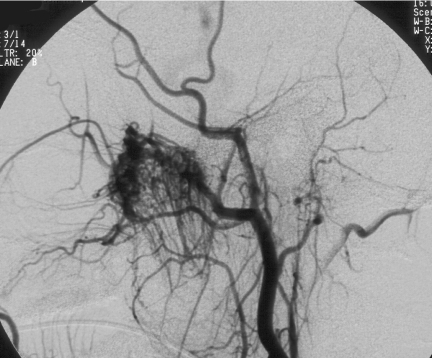
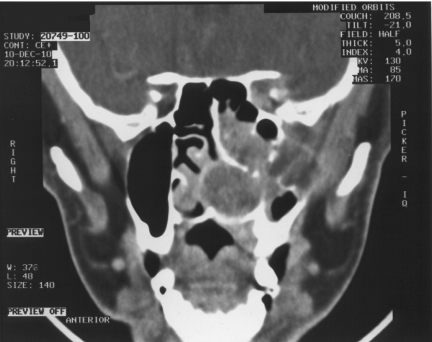
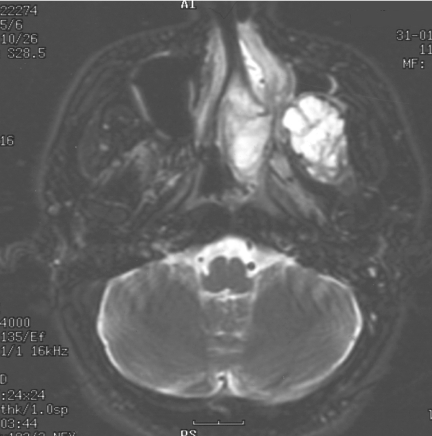
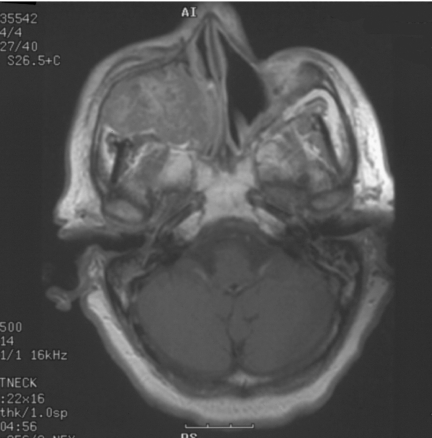
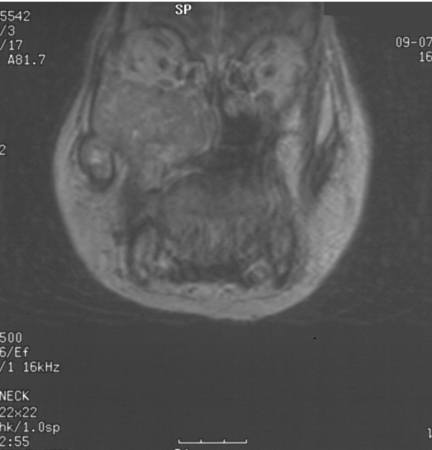
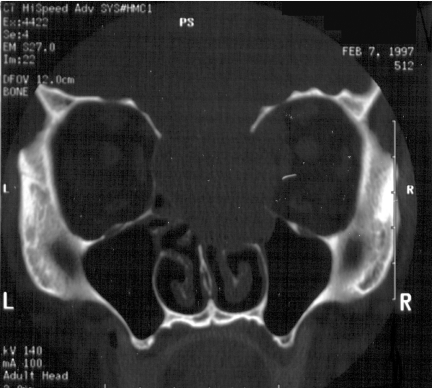
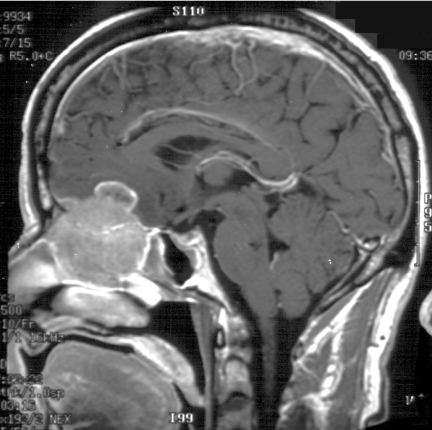
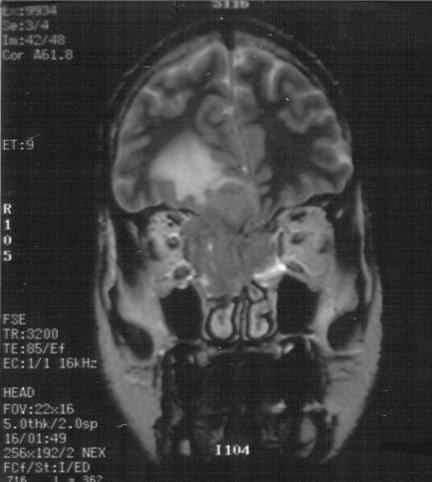
Sinonasal disease is one of the most common clinical head and neck pathologies. The majority of sinonasal pathology is inflammatory with neoplasms comprising approximately 3% of all head and neck tumours. Although sinus tumours are rare, they portend a poor prognosis, often due to advanced disease at diagnosis. Like most neoplasms, early detection improves prognosis, therefore clinicians and radiologists should be aware of features separating tumours from inflammatory sinus disease. This article reviews the anatomy, clinical features, imaging findings, treatment and histopathology of selected sinonasal tumours. Benign neoplasms reviewed include osteoma, inverting papilloma, and juvenile nasal angiofibroma. Malignant neoplasms reviewed include squamous cell carcinoma, the minor salivary gland tumour, adenoid cystic carcinoma, adenocarcinoma, melanoma, lymphoma, and olfactory neuroblastoma (esthesioneuroblastoma).
International Cancer Imaging Society.
Figures






References
-
- Som P. Tumors and tumorlike conditions of the sinonasal cavity. In: Som P, Bergeron RT, editors. Head and Neck Imaging. 2nd ed. St. Louis: Mosby-Year Book; 1990. pp. 169–227.
-
- Boring CC, Squires TS, Tong T. Cancer statistics. CA Cancer J Clin. 1992;42:19–38. - PubMed
-
- Som PM, Dillon WP, Sze G, et al. Benign and malignant sinonasal lesions with intracranial extension:differentiation with MR imaging. Radiology. 1989;172:763–6. - PubMed
-
- Namdar I, Edelstein DR, Huo J, Lazar A, Kimmelman CP, Soletic R. Management of osteomas of the paranasal sinuses. Am J Rhinol. 1998;12:393–8. - PubMed
-
- Rappaport JM, Attia EL. Pneumocephalus in frontal sinus osteoma: a case report. J Otolaryngol. 1994;23:430–6. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources