

Diagnosis and treatment of nontuberculous mycobacterial pulmonary diseases: a Korean perspective
- PMID: 16361797
- PMCID: PMC2779319
- DOI: 10.3346/jkms.2005.20.6.913
Diagnosis and treatment of nontuberculous mycobacterial pulmonary diseases: a Korean perspective
Abstract
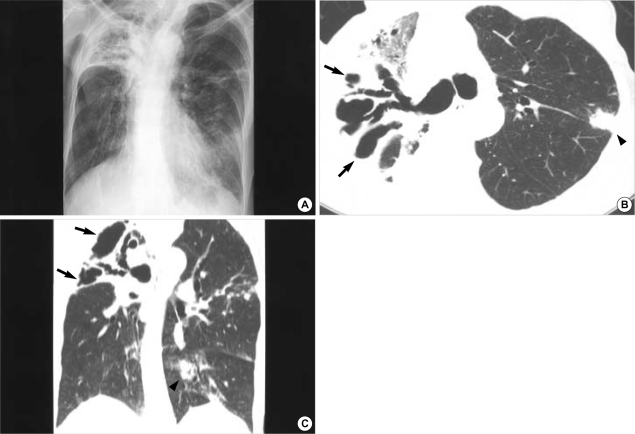
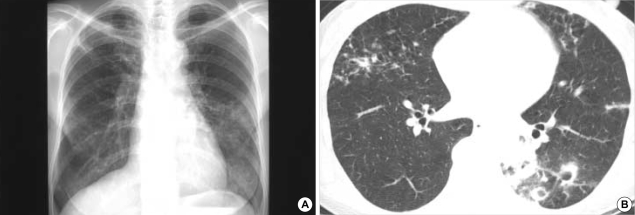
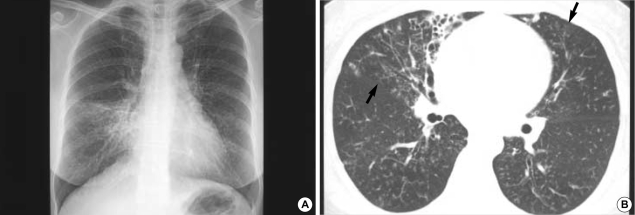
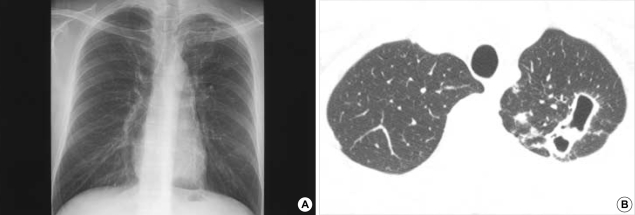
The incidence of pulmonary disease caused by nontuberculous mycobacteria (NTM) appears to be increasing worldwide. In Korea, M. avium complex and M. abscessus account for most of the pathogens encountered, whilst M. kansasii is a relatively uncommon cause of NTM pulmonary diseases. NTM pulmonary disease is highly complex in terms of its clinical presentation and management. Because its clinical features are indistinguishable from those of pulmonary tuberculosis and NTMs are ubiquitous in the environment, the isolation and identification of causative organisms are mandatory for diagnosis, and some specific diagnostic criteria have been proposed. The treatment of NTM pulmonary disease depends on the infecting species, but decisions concerning the institution of treatment are never easy. Treatment requires the use of multiple drugs for 18 to 24 months. Thus, treatment is expensive, often has significant side effects, and is frequently not curative. Therefore, clinicians should be confident that there is sufficient pathology to warrant prolonged, multidrug treatment regimens. In all of the situations, outcomes can be best optimized only when clinicians, radiologists, and laboratories work cooperatively.
Figures
References
-
- Hale YM, Pfyffer GE, Salfinger M. Laboratory diagnosis of mycobacterial infections: new tools and lessons learned. Clin Infect Dis. 2001;33:834–846. - PubMed
-
- American Thoracic Society. Diagnosis and treatment of disease caused by nontuberculous mycobacteria. Am J Respir Crit Care Med. 1997;156:S1–S25. - PubMed
-
- Koh WJ, Kwon OJ. Treatment of nontuberculous mycobacterial pulmonary diseases. Tuberc Respir Dis. 2004;56:5–17.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
