

Laparoscopic surgery may be associated with severe pain and high analgesia requirements in the immediate postoperative period
- PMID: 16371735
- PMCID: PMC1449966
- DOI: 10.1097/01.sla.0000193806.81428.6f
Laparoscopic surgery may be associated with severe pain and high analgesia requirements in the immediate postoperative period
Abstract
Objective: To assess the immediate (0-4 hours) postoperative pain level in patients after laparoscopy and laparotomy whose analgesic requirement in the Post-Anesthesia Care Unit (PACU) exceeds standard morphine therapy.
Background data: Clinical observation has raised the suspicion that laparoscopic surgery may be associated with more intense immediate postoperative pain than expected.
Methods: This prospective study assessed the 24-hour pain intensity and analgesia requirements in patients who underwent similar abdominal surgery via laparoscopy or laparotomy under standardized general anesthesia and whose pain in the PACU was resistant to 120 microg/kg intravenous morphine.
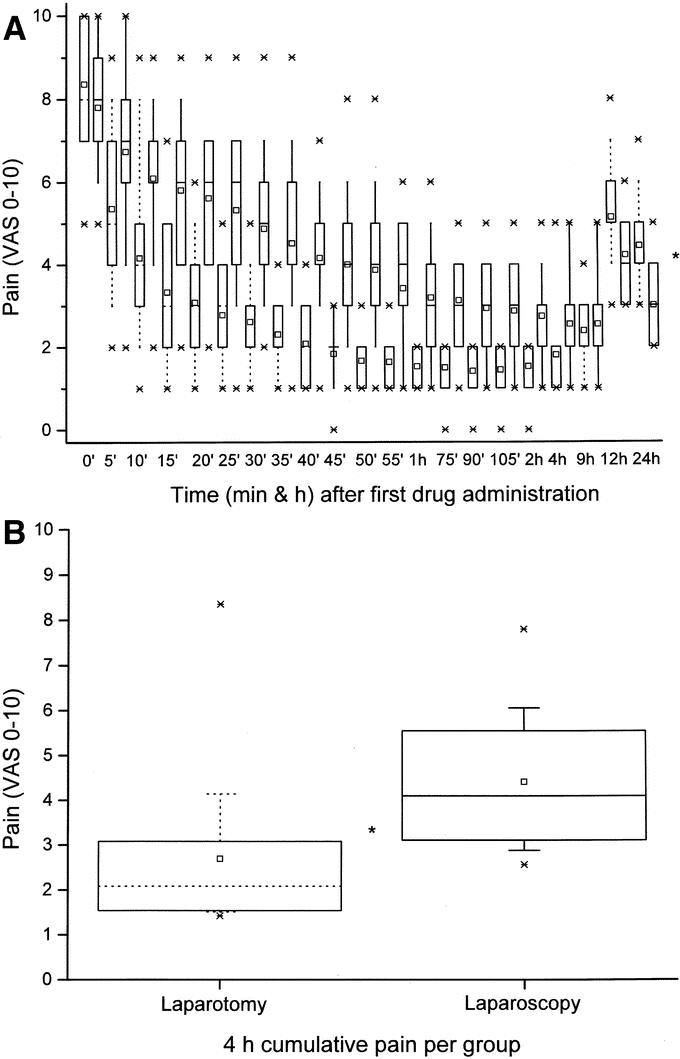
Results: Of 145 sampled PACU patients, 67 were in pain (> or =6 of 10 VAS) within a 30-minute postoperative period. They were then given up to 4 intravenous boluses of 15 microg/kg morphine + 250 microg/kg ketamine. The pain VAS of 36 laparotomy patients was 4.14 +/- 2.14 (SD) and 1.39 +/- 0.55 at 10 and 120 minutes, respectively, after 1.33 +/- 0.59 doses of morphine + ketamine; the pain VAS of 31 laparoscopy patient was 6.06 +/- 1.75 and 2.81 +/- 1.14, respectively (P < 0.0005) following 2.0 +/- 0.53 doses (P = 0.0005). Diclofenac 75 mg intramuscular usage was similar (P = 0.43) between the groups up to 9 hours after surgery but was higher in the laparotomy group by 24 hours (P = 0.01). Pain scores at 24 hours after surgery were lower for the laparoscopy patients (3.01 +/- 0.87) compared with their laparotomy counterparts (4.45 +/- 0.98, P < 0.001).
Conclusions: Among patients after abdominal surgery with severe immediate (0-4 hours) postoperative pain, laparoscopic patients are a significant (46%) proportion, and their pain is more intense, requiring more analgesics than painful patients (54%) do after laparotomy. By 24 hours, the former are in less pain than the latter.
Figures
References
-
- Schwenk W, Bohm B, Muller JM. Postoperative pain and fatigue after laparoscopic or conventional colorectal resections: a prospective randomized trial. Surg Endosc. 1998;12:1131–1136. - PubMed
-
- Vara-Thorbeck C, Garcia-Caballero M, Salvi M, et al. Indications and advantages of laparoscopy-assisted colon resection for carcinoma in elderly patients. Surg Laparosc Endosc. 1994;4:110–118. - PubMed
-
- Mais V, Ajossa S, Guerriero S, et al. Laparoscopic versus abdominal myomectomy: a prospective, randomized trial to evaluate benefits in early outcome. Am J Obstet Gynecol. 1996;174:654–658. - PubMed
-
- Ortega AE, Peters JH, Incarbone R, et al. A prospective randomized comparison of the metabolic and stress hormonal responses of laparoscopic and open cholecystectomy. J Am Coll Surg. 1996;183:249–256. - PubMed
-
- Weinbroum AA. A single small dose of postoperative ketamine provides rapid and sustained improvement in morphine analgesia in the presence of morphine-resistant pain. Anesth Analg. 2003;96:789–795. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
