

Lymphovascular invasion is associated with poor survival in gastric cancer: an application of gene-expression and tissue array techniques
- PMID: 16371738
- PMCID: PMC1449982
- DOI: 10.1097/01.sla.0000194087.96582.3e
Lymphovascular invasion is associated with poor survival in gastric cancer: an application of gene-expression and tissue array techniques
Abstract
Objectives: To examine a population-based cohort for the association between clinicopathologic predictors of survival and immunohistochemical markers (IHC), and to assess changes in gene expression that are associated with lymphovascular invasion (LVI).
Summary background data: LVI has been associated with poor survival and aggressive tumor behavior. The molecular changes responsible for the behavior of gastric cancer have yet to be determined. Characterization of IHC markers and gene expression profiles may identify molecular alterations governing tumor behavior.
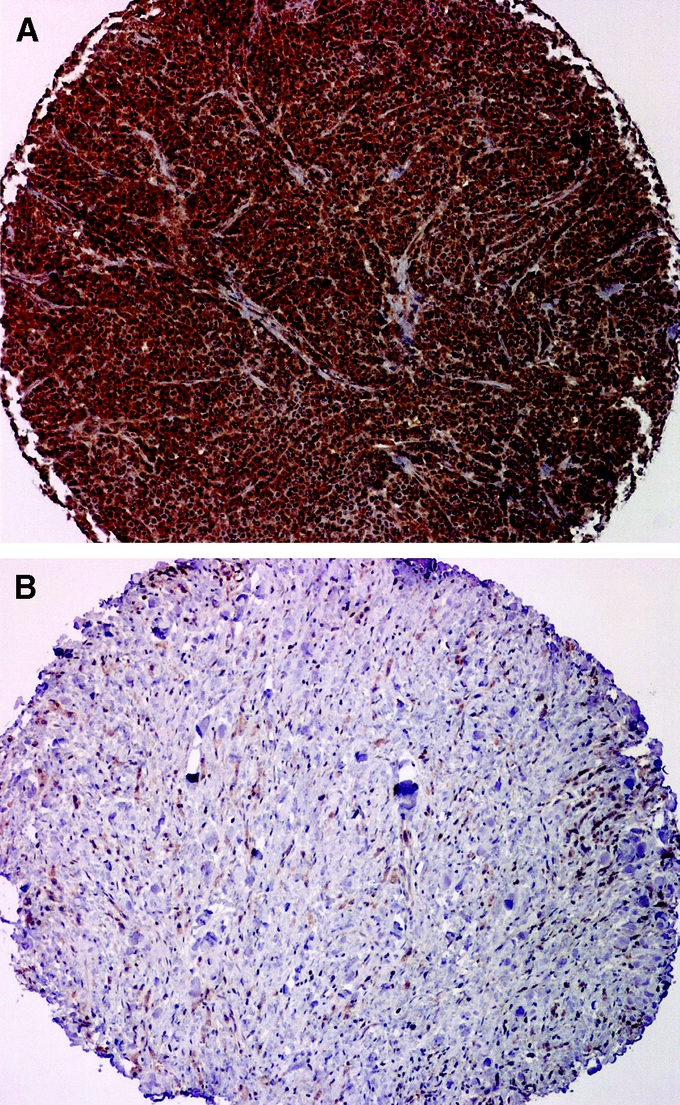
Methods: : Clinicopathologic and survival data of 114 patients were reviewed. Archival specimens were used to construct a multitumor tissue array that was subjected to IHC of selected protein targets. Correlation of IHC with tumor thickness (T status), LVI and prognosis was studied. Microarray analysis of fresh gastric cancer tissue was conducted to examine the gene expression profile with respect to LVI.
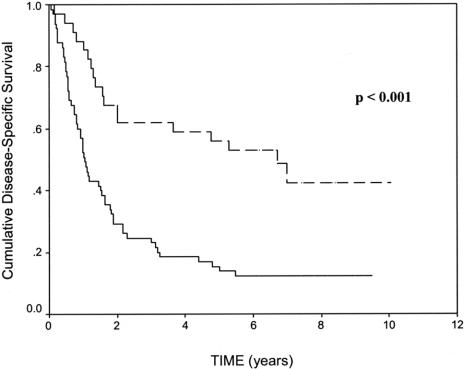
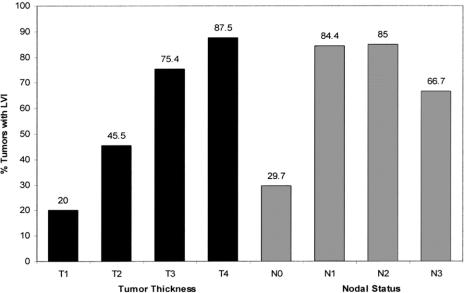
Results: In a multivariate analysis, nodal status (N), metastasis (M), and LVI were independent predictors of survival. LVI was associated with a 5-year survival of 13.9% versus 55.9% in patients in whom it was absent. LVI correlated with advancing T status (P = 0.001) and N status (P < 0.001). IHC staining of cyclooxygenase-2 (COX-2) correlated with T status, tumor grade, lymph node positivity, and IHC staining of matrix metalloproteinase-2 (MMP-2) and matrix metalloproteinase-9 (MMP-9). Microarray analyses suggested differential expression of oligophrenin-1 (OPHN1) and ribophorin-II (RPNII) with respect to LVI.
Conclusion: LVI was an independent predictor of survival in gastric cancer. Expression of COX-2 may facilitate tumor invasion through MMP-2 and MMP-9 activation. OPHN1 and RPN II appeared to be differentially expressed in gastric cancers exhibiting LVI. The reported function of OPHN1 and RPN II makes these gene products promising candidates for future studies involving LVI in gastric cancer.
Figures

Similar articles
-
Gastric cancer: establishing predictors of biologic behavior with use of population-based data.Ann Surg Oncol. 2004 Jun;11(6):629-35. doi: 10.1245/ASO.2004.09.002. Epub 2004 May 18. Ann Surg Oncol. 2004. PMID: 15150070
-
Reevaluation of lymphovascular invasion in gastric cancer using endothelial markers D2-40 and EVG: Enhanced detection, better predictor of lymph node metastasis and biological aggressiveness.J Surg Oncol. 2021 May;123(8):1736-1741. doi: 10.1002/jso.26468. Epub 2021 Mar 26. J Surg Oncol. 2021. PMID: 33772776
-
Impact of Lymphovascular Invasion on Survival Outcome in Patients With Gastric Cancer.Am J Clin Pathol. 2020 May 5;153(6):833-841. doi: 10.1093/ajcp/aqaa021. Am J Clin Pathol. 2020. PMID: 32146483
-
Overexpression of twist and matrix metalloproteinase-9 with metastasis and prognosis in gastric cancer.Asian Pac J Cancer Prev. 2013;14(9):5055-60. doi: 10.7314/apjcp.2013.14.9.5055. Asian Pac J Cancer Prev. 2013. PMID: 24175775
-
Lymphovascular invasion and nodal metastasis in intramucosal adenocarcinoma of the esophagus and esophagogastric junction.J Dig Dis. 2015 Apr;16(4):197-204. doi: 10.1111/1751-2980.12230. J Dig Dis. 2015. PMID: 25620066 Review.
Cited by
-
Impact of Altered Body Composition on Clinical and Oncological Outcomes in Intrahepatic Cholangiocarcinoma.J Clin Med. 2023 Dec 18;12(24):7747. doi: 10.3390/jcm12247747. J Clin Med. 2023. PMID: 38137817 Free PMC article.
-
Impact of capillary invasion on the prognosis of gastric adenocarcinoma patients: A retrospective cohort study.Oncotarget. 2016 May 24;7(21):31215-25. doi: 10.18632/oncotarget.9101. Oncotarget. 2016. PMID: 27145279 Free PMC article.
-
Impact of lymphatic and/or blood vessel invasion in stage II gastric cancer.World J Gastroenterol. 2012 Jul 21;18(27):3610-6. doi: 10.3748/wjg.v18.i27.3610. World J Gastroenterol. 2012. PMID: 22826628 Free PMC article.
-
Characterizing Lymphovascular Invasion in Pediatric and Adolescent Malignant Ovarian Nongerminomatous Germ Cell Tumors: A Report from the Children's Oncology Group.J Pediatr Surg. 2023 Dec;58(12):2399-2404. doi: 10.1016/j.jpedsurg.2023.08.008. Epub 2023 Aug 22. J Pediatr Surg. 2023. PMID: 37699777 Free PMC article.
-
Evaluation of Lymphovascular Invasion by CD31 Expression in Gastric Adenocarcinoma.Iran J Pathol. 2023 Spring;18(2):140-146. doi: 10.30699/ijp.2023.562466.2977. Epub 2023 Jun 20. Iran J Pathol. 2023. PMID: 37600573 Free PMC article.
References
-
- Volpe CM, Driscoll DL, Douglass HO Jr. Outcome of patients with proximal gastric cancer depends on extent of resection and number of resected lymph nodes. Ann Surg Oncol. 2000;7:139–144. - PubMed
-
- Msika S, Benhamiche A, Jouve J-L, et al. Prognostic factors after curative resection of gastric cancer: a population-based study. Eur J Cancer. 2000;36:390–396. - PubMed
-
- Talamonti MS, Kim SP, Yao KA, et al. Surgical outcomes of patients with gastric carcinoma: the importance of primary tumor location and microvessel invasion. Surgery. 2003;134:720–727; discussion 727–729. - PubMed
-
- Hundahl SA, Phillips JL, Menck HR. The National Cancer Data Base Report on poor survival of U.S. gastric carcinoma patients treated with gastrectomy: Fifth Edition American Joint Committee on Cancer staging, proximal disease, and the ‘different disease’ hypothesis. Cancer. 2000;88:921–932. - PubMed
-
- Chambers WM, Khan U, Gagliano A, et al. Tumour morphology as a predictor of outcome after local excision of rectal cancer. Br J Surg. 2004;91:457–459. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
