

A clinical outcome-based prospective study on venous thromboembolism after cancer surgery: the @RISTOS project
- PMID: 16371741
- PMCID: PMC1449979
- DOI: 10.1097/01.sla.0000193959.44677.48
A clinical outcome-based prospective study on venous thromboembolism after cancer surgery: the @RISTOS project
Abstract
Summary background data: The epidemiology of venous thromboembolism (VTE) after cancer surgery is based on clinical trials on VTE prophylaxis that used venography to screen deep vein thrombosis (DVT). However, the clinical relevance of asymptomatic venography-detected DVT is unclear, and the population of these clinical trials is not necessarily representative of the overall cancer surgery population.
Objective: The aim of this study was to evaluate the incidence of clinically overt VTE in a wide spectrum of consecutive patients undergoing surgery for cancer and to identify risk factors for VTE.
Methods: @RISTOS was a prospective observational study in patients undergoing general, urologic, or gynecologic surgery. Patients were assessed for clinically overt VTE occurring up to 30 +/- 5 days after surgery or more if the hospital stay was longer than 35 days. All outcome events were evaluated by an independent Adjudication Committee.
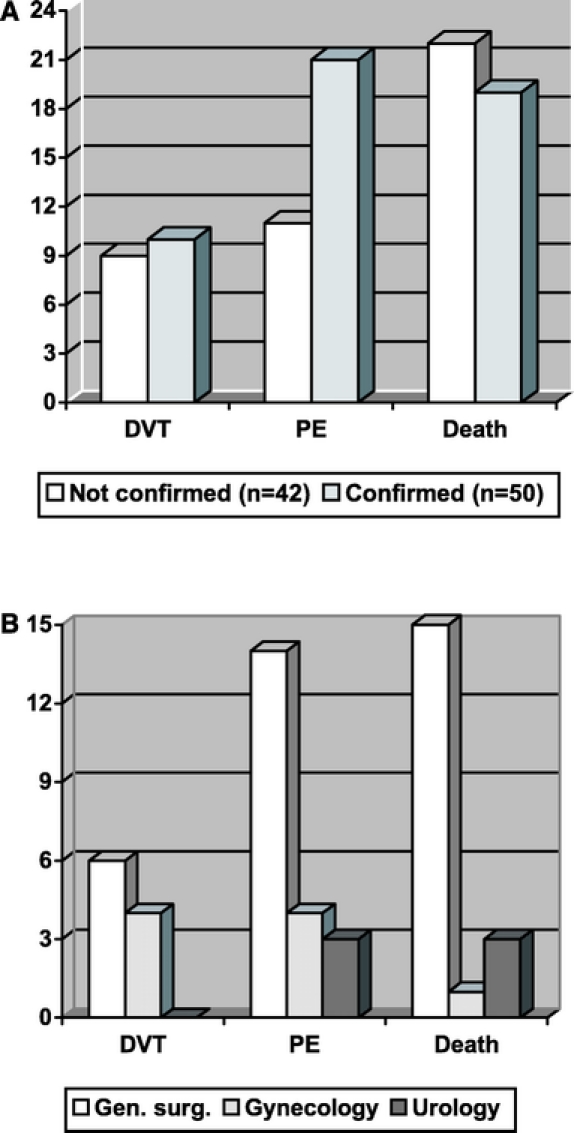
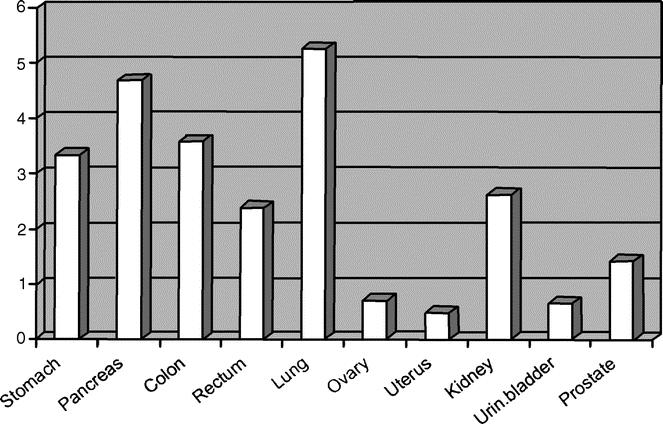
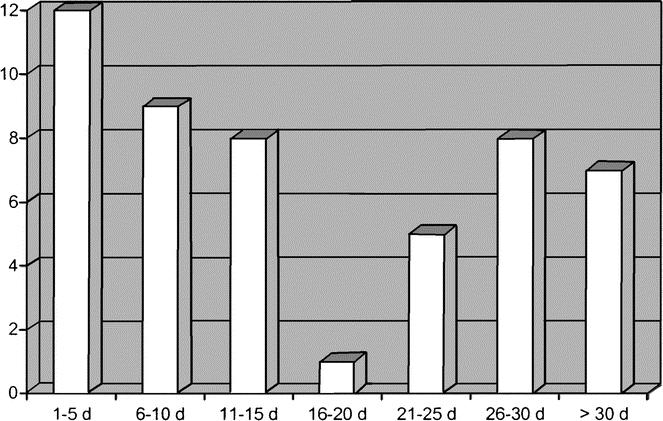
Results: A total of 2373 patients were included in the study: 1238 (52%) undergoing general, 685 (29%) urologic, and 450 (19%) gynecologic surgery. In-hospital prophylaxis was given in 81.6% and postdischarge prophylaxis in 30.7% of the patients. Fifty patients (2.1%) were adjudicated as affected by clinically overt VTE (DVT, 0.42%; nonfatal pulmonary embolism, 0.88%; death 0.80%). The incidence of VTE was 2.83% in general surgery, 2.0% in gynecologic surgery, and 0.87% in urologic surgery. Forty percent of the events occurred later than 21 days from surgery. The overall death rate was 1.72%; in 46.3% of the cases, death was caused by VTE. In a multivariable analysis, 5 risk factors were identified: age above 60 years (2.63, 95% confidence interval, 1.21-5.71), previous VTE (5.98, 2.13-16.80), advanced cancer (2.68, 1.37-5.24), anesthesia lasting more than 2 hours (4.50, 1.06-19.04), and bed rest longer than 3 days (4.37, 2.45-7.78).
Conclusions: VTE remains a common complication of cancer surgery, with a remarkable proportion of events occurring late after surgery. In patients undergoing cancer surgery, VTE is the most common cause of death at 30 days after surgery.
Figures
Comment in
-
Commentary. A clinical outcome-based prospective study on venous thromboembolism after cancer surgery: the @RISTOS Project.Perspect Vasc Surg Endovasc Ther. 2006 Dec;18(4):343-4. Perspect Vasc Surg Endovasc Ther. 2006. PMID: 17396360 No abstract available.
References
-
- Kakkar VV, Howe CT, Nicolaides AN, et al. Deep vein thrombosis of the leg: is there a ‘high risk’ group? Am J Surg. 1970;120:527–530. - PubMed
-
- Walsh JJ, Bonnar J, Wright FW. A study of pulmonary embolism and deep leg vein thrombosis after major gynaecologic surgery using labelled fibrinogen phlebography and lung scanning. J Obstet Gynaecol Br Commonw. 1974;81:311–316. - PubMed
-
- Huber O, Bounameux H, Borst F, et al. Postoperative pulmonary embolism after hospital discharge: an underestimated risk. Arch Surg. 1992;127:310–313. - PubMed
-
- Gallus AS. Prevention of post-operative deep leg vein thrombosis in patients with cancer. Thromb Haemost. 1997;78:126–132. - PubMed
-
- Geerts WH, Pineo JF, Heit JA, et al. Prevention of venous thromboembolism: the seventh ACCP conference on antithrombotic and thrombolytic therapy. Chest. 2004;126(suppl):338–400. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
