

The treatment of acute infectious conjunctivitis with fusidic acid: a randomised controlled trial
- PMID: 16378561
- PMCID: PMC1570507
The treatment of acute infectious conjunctivitis with fusidic acid: a randomised controlled trial
Abstract
Background: Acute infectious conjunctivitis is a common disorder in primary care. Despite a lack of evidence regarding the effectiveness of topical antibiotics for the treatment of acute infectious conjunctivitis, most patients presenting in primary care with the condition receive topical antibiotics. In The Netherlands, fusidic acid is most frequently prescribed.
Aim: To assess the effectiveness of fusidic acid gel compared to placebo for acute infectious conjunctivitis.
Design: Double-blind randomised placebo-controlled trial.
Setting: Twenty-five Dutch primary care centres.
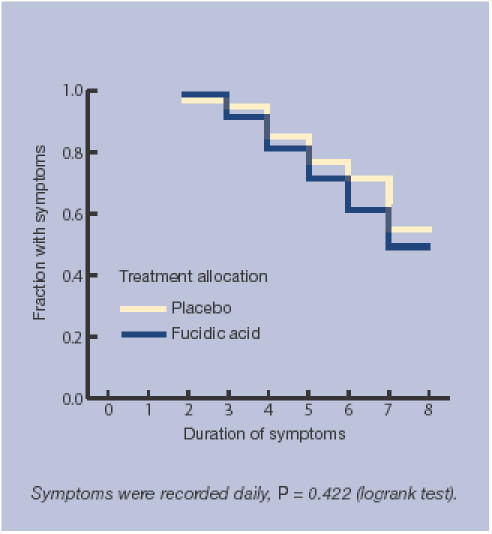
Method: Adults presenting with a red eye and either (muco)purulent discharge or glued eyelid(s) were allocated to either one drop of fusidic acid gel 1% or placebo, four times daily during one week. The main outcome measure was the difference in recovery rates at 7 days. Secondary outcome measures were difference in bacterial eradication rates, a survival time analysis of the duration of symptoms, and the difference in recovery rates in culture-positive and culture-negative patients.
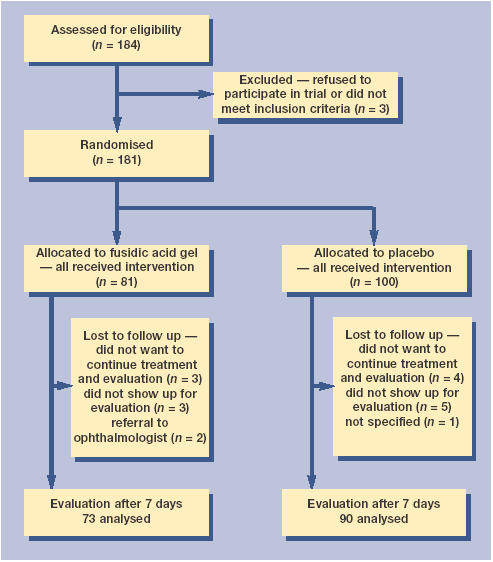
Results: One hundred and eighty-one patients were randomised and 163 patients were analysed. Forty-five of the 73 patients in the treatment and 53 of the 90 patients in the placebo group recovered (adjusted risk difference = 5.3% [95% confidence interval {CI} = -11 to 18]). There was no difference between the median duration of symptoms in the two groups. At baseline, the prevalence of a positive bacterial culture was 32% (58/181). The bacterial eradication rate was 76% in the treatment and 41% in the placebo group (risk difference = 35% [95% CI = 9.3 to 60.4]). In culture positive patients, the treatment effect tended to be strong (adjusted risk difference = 23% [95% CI = -6 to 42]).
Conclusion: At 7 days, cure rates in the fusidic acid gel and placebo group were similar, but the confidence interval was too wide to clearly demonstrate their equivalence. These findings do not support the current prescription practices of fusidic acid by GPs.
Figures
References
-
- Blom GH, Cleveringa JP, Louisse AC, et al. NHG Standaard Het rode oog [NHG Practice Guideline ‘The Red Eye’] Huisarts Wet. 1996;39:225–238.
-
- Okkes IM, Oskam SK, Lamberts H. Van klacht naar diagnose. Episodegegevens uit de huisartspraktijk. Bussum: Coutinho; 1998. [From complaint to diagnosis. Episodic data from general practice]
-
- Van der Werf GT, Smit RJA, Stewart RE, Meyboom-de Jong B. Spiegel op de huisarts: over registratie van ziekte, medicatie en verwijzing in de geautomatiseerde huisartspraktijk. Groningen: Rijksuniversiteit Groningen; 1998. [Reflection on the general practitioner: about registration of illness, medication, and referrals in the computerised general practice]
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical