

Using simulation to estimate the cost effectiveness of improving ambulance and thrombolysis response times after myocardial infarction
- PMID: 16381082
- PMCID: PMC2564138
- DOI: 10.1136/emj.2004.023036
Using simulation to estimate the cost effectiveness of improving ambulance and thrombolysis response times after myocardial infarction
Abstract
Objectives: To quantify the health gains and costs associated with improving ambulance and thrombolysis response times for acute myocardial infarction.
Design: A computer simulation model. PATIENTS/SETTINGS: Patients experiencing acute myocardial infarction in England.
Interventions: Improving the ambulance response time to 75% of calls reached within 8 minutes and the hospital arrival to thrombolysis time interval (door-to-needle time) to 75% receiving it within 30 minutes and 20 minutes, compared to best estimates of response times in the mid-1990s.
Main outcome measures: Deaths prevented, life years saved, and discounted cost per life year saved.
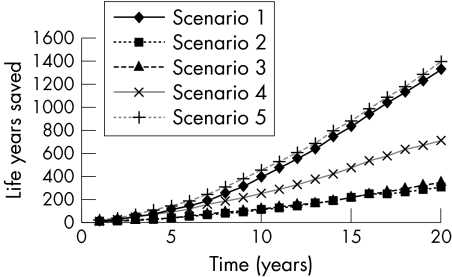
Results: Improving the ambulance response to 75% of calls within 8 minutes resulted in an estimate of 5 deaths prevented or 57 life years saved per million population per year, with a discounted incremental cost per life year saved of 8540 pounds sterling over 20 years. The corresponding benefit of improving the door-to-needle time to 75% of myocardial infarction patients within 30 minutes was an estimated 2 deaths prevented and 15 life years saved per million population per year, with a discounted incremental cost per life year saved of between 10,150 pounds sterling to 54,230 pounds sterling over 20 years. Little further gain was associated with reaching the 20 minute target. Combining ambulance and thrombolysis targets resulted in 70 life years saved per million population per year.
Conclusions: Improving ambulance response times appears to be cost effective. Reducing door-to-needle time will have a smaller effect at an uncertain cost. Further benefits may be gained from reducing the time from onset of symptoms to starting thrombolysis.
Conflict of interest statement
Competing interests: TQ is a member of an advisory board for Boehringer Ingelheim.
References
-
- Fibrinolytic Therapy Trialists' Collaborative Group Indications for fibrinolytic therapy in suspected acute myocardial infarction: collaborative overview of early mortality and major morbidity results from all randomised trials of more than 1000 patients. Lancet 1994343311–322. - PubMed
-
- Keeley E C, Boura J A, Gruines C L. Primary angioplasty versus intravenous thrombolytic therapy for acute myocardial infarction: a quantitative review of 23 randomised trials. Lancet 200336113–20. - PubMed
-
- Department of Health National service framework for coronary heart disease: modern standards and service models. London: Department of Health, 2000
-
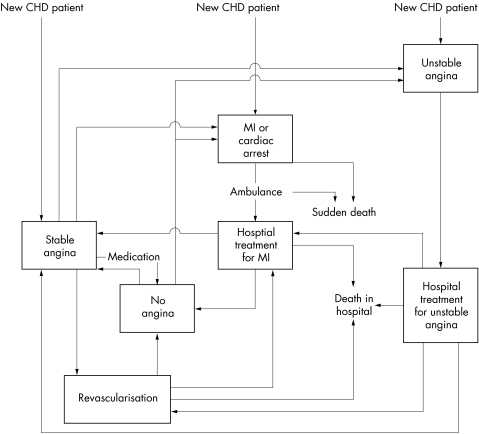
- Cooper K, Davies R, Roderick P.et al The development of a simulation model of the treatment of coronary heart disease. Health Care Manage Sci 2002259–67. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical