

Anatomic basis of sharp pelvic dissection for curative resection of rectal cancer
- PMID: 16385648
- PMCID: PMC2810586
- DOI: 10.3349/ymj.2005.46.6.737
Anatomic basis of sharp pelvic dissection for curative resection of rectal cancer
Abstract
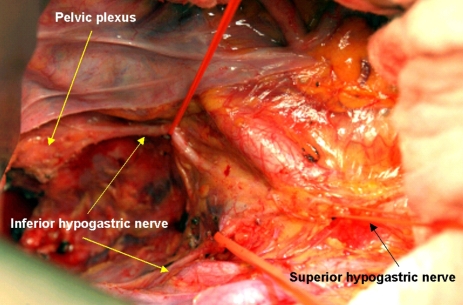
The optimal goals in the surgical treatment of rectal cancer are curative resection, anal sphincter preservation, and preservation of sexual and voiding functions. The quality of complete resection of rectal cancer and the surrounding mesorectum can determine the prognosis of patients and their quality of life. With the emergence of total mesorectal excision in the field of rectal cancer surgery, anatomical sharp pelvic dissection has been emphasized to achieve these therapeutic goals. In the past, the rates of local recurrence and sexual/voiding dysfunction have been high. However, with sharp pelvic dissection based on the pelvic anatomy, local recurrence has decreased to less than 10%, and the preservation rate of sexual and voiding function is high. Improved surgical techniques have created much interest in the surgical anatomy related to curative rectal cancer surgery, with particular focus on the fascial planes and nerve plexuses and their relationship to the surgical planes of dissection. A complete understanding of rectum anatomy and the adjacent pelvic organs are essential for colorectal surgeons who want optimal oncologic outcomes and safety in the surgical treatment of rectal cancer.
Figures
References
-
- NIH consensus conference. Adjuvant therapy for patients with colon and rectal cancer. JAMA. 1990;264:1444–1450. - PubMed
-
- Maurer CA, Z'Graggen K, Renzulli P, Schilling MK, Netzer P, Buchler MW. Total mesorectal excision preserves male genital function compared with conventional rectal cancer surgery. Br J Surg. 2001;88:1501–1505. - PubMed
-
- Heald RJ, Husband EM, Ryall RD. The mesorectum in rectal cancer surgery-the clue to pelvic recurrence? Br J Surg. 1982;69:613–616. - PubMed
-
- Heald RJ, Ryall RD. Recurrence and survival after total mesorectal excision for rectal cancer. Lancet. 1986;1:1479–1482. - PubMed
-
- MacFarlane JK, Ryall RD, Heald RJ. Mesorectal excision for rectal cancer. Lancet. 1993;341:457–460. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
