

Prognostic value of ventricular arrhythmias and heart rate variability in patients with unstable angina
- PMID: 16387812
- PMCID: PMC1861090
- DOI: 10.1136/hrt.2005.070714
Prognostic value of ventricular arrhythmias and heart rate variability in patients with unstable angina
Abstract
Objectives: To assess the prognostic value of ventricular arrhythmias (VA) and heart rate variability (HRV) in patients with unstable angina.
Design: Multicentre prospective study.
Setting: 17 cardiological centres in Italy.
Patients: 543 consecutive patients with unstable angina and preserved left ventricular function (ejection fraction >or=40%) enrolled in the SPAI (Stratificazione Prognostica dell'Angina Instabile) study.
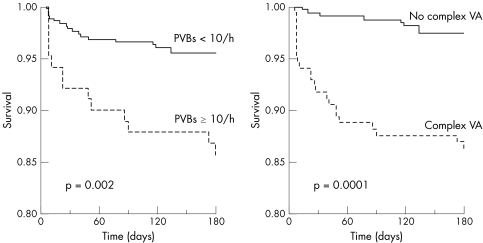
Methods: Patients underwent 24 h ECG Holter monitoring within 24 h of hospital admission. Tested variables were frequent ventricular extrasystoles (>or=10/h), complex (that is, frequent or repetitive) VA, and bottom quartile values of time-domain and frequency-domain HRV variables. Primary end points were in-hospital and six-month total and cardiac deaths.
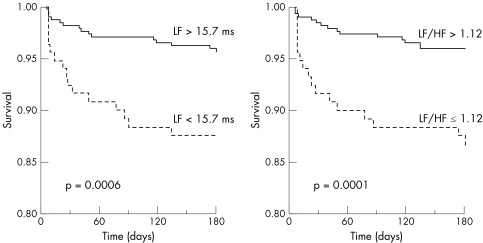
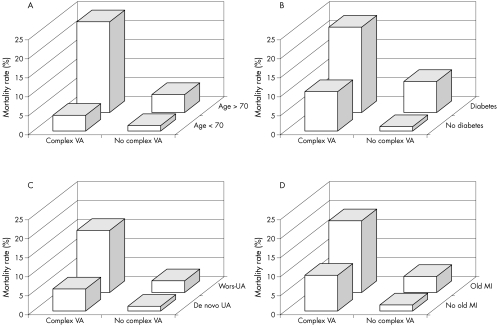
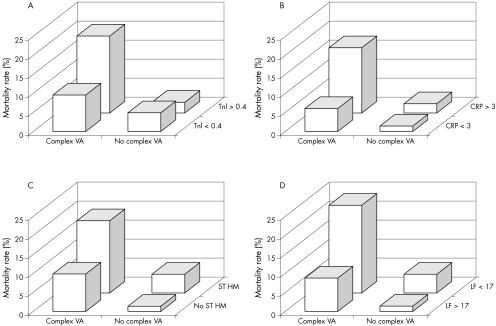
Results: Eight patients died in hospital (1.5%) and 32 (5.9%, 29 cardiac) during follow up. Both complex VA and frequent extrasystoles were strongly predictive of death in hospital and at follow up, even after adjustment for clinical (age, sex, cardiac risk factors and history of myocardial infarction) and laboratory (troponin I, C reactive protein and transient myocardial ischaemia on Holter monitoring) variables. At univariate analysis bottom quartile values of three HRV variables (standard deviation of RR intervals index, low-frequency amplitude and low to high frequency ratio) were associated with in-hospital death, and bottom quartile values of most HRV variables predicted six-month fatal events. At multivariate Cox survival analysis reduced low-frequency amplitude was consistently found to be independently associated with fatal end points.
Conclusion: In patients with unstable angina with preserved myocardial function, both VA and HRV are independent predictors of in-hospital and medium-term mortality, suggesting that these factors should be taken into account in the risk stratification of these patients.
Similar articles
-
Relation of heart rate variability to serum levels of C-reactive protein in patients with unstable angina pectoris.Am J Cardiol. 2006 Jun 15;97(12):1702-6. doi: 10.1016/j.amjcard.2006.01.029. Epub 2006 Apr 21. Am J Cardiol. 2006. PMID: 16765117
-
[The predictive value for major arrhythmic events of ventricular arrhythmias, particularly nonsustained ventricular tachycardias, in the subacute phase of a fibrinolyzed infarct. An analysis of GISSI-2 data. Gruppo Italiano per lo Studio della Streptochinasi nell'Infarto Miocardico].G Ital Cardiol. 1995 Jan;25(1):77-87. G Ital Cardiol. 1995. PMID: 7642014 Clinical Trial. Italian.
-
Two year follow-up of cardiac mortality and recurrent cardiac events in patients after acute myocardial infarction or unstable angina.Croat Med J. 1998 Dec;39(4):407-11. Croat Med J. 1998. PMID: 9841941
-
[Rationale, characteristics and study design of PREAMI (Perindopril and Remodelling in the Elderly with Acute Myocardial Infraction)].Ital Heart J. 2005 Nov;6 Suppl 7:14S-23S. Ital Heart J. 2005. PMID: 16485513 Review. Italian.
-
Identification of patients with high risk of arrhythmic mortality. Role of ambulatory monitoring, signal-averaged ECG, and heart rate variability.Cardiol Clin. 1993 Feb;11(1):55-63. Cardiol Clin. 1993. PMID: 8435824 Review.
Cited by
-
Very Low Frequency Heart Rate Variability Predicts the Development of Post-Stroke Infections.Transl Stroke Res. 2019 Dec;10(6):607-619. doi: 10.1007/s12975-018-0684-1. Epub 2019 Jan 7. Transl Stroke Res. 2019. PMID: 30617993
-
Sleep heart rate variability assists the automatic prediction of long-term cardiovascular outcomes.Sleep Med. 2020 Mar;67:217-224. doi: 10.1016/j.sleep.2019.11.1259. Epub 2019 Dec 16. Sleep Med. 2020. PMID: 31972509 Free PMC article.
-
Machine learning-based predictive modeling of angina pectoris in an elderly community-dwelling population: Results from the PoCOsteo study.PLoS One. 2025 Aug 5;20(8):e0329023. doi: 10.1371/journal.pone.0329023. eCollection 2025. PLoS One. 2025. PMID: 40763138 Free PMC article.
-
Autonomic dysfunction and risk stratification assessed from heart rate pattern.Open Neurol J. 2010 Jun 15;4:39-49. doi: 10.2174/1874205X01004010039. Open Neurol J. 2010. PMID: 21258571 Free PMC article.
-
Effects of coronary revascularization by elective percutaneous coronary intervention on cardiac autonomic modulation assessed by heart rate variability: a single-center prospective cohort study.Am J Cardiovasc Dis. 2021 Feb 15;11(1):164-175. eCollection 2021. Am J Cardiovasc Dis. 2021. PMID: 33815932 Free PMC article.
References
-
- Bigger J T, Weld F M, Rolnitzki L M. Prevalence, characteristics and significance of ventricular tachycardia (three or more complexes) detected with ambulatory electrocardiographic recording in the late hospital phase of acute myocardial infarction. Am J Cardiol 198148815–823. - PubMed
-
- Kostis J B, Friedman L M, Goldstein S, for the BHATB Study Group et al Prognostic significance of ventricular ectopic activity in survivors of acute myocardial infarction. J Am Coll Cardiol 198710231–242. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials