

Limited predictability of amikacin clearance in extreme premature neonates at birth
- PMID: 16390350
- PMCID: PMC1884978
- DOI: 10.1111/j.1365-2125.2005.02530.x
Limited predictability of amikacin clearance in extreme premature neonates at birth
Abstract
Aim: Identify and quantify factors describing variability of amikacin clearance in preterm neonates at birth.
Methods: Population pharmacokinetics of amikacin were estimated in a cohort of 205 extreme preterm neonates [post conception age (PCA) 27.8, SD 1.8, range 24-30 weeks; weight 1.07, SD 0.34, range 0.45-1.98 kg, postnatal age < 72 h]. Covariate analysis included weight, PCA, Apgar score, prophylactic administration of a nonsteroidal anti-inflammatory drug (NSAID) to the neonate, maternal indomethacin and betamethasone administration, and chorioamnionitis.
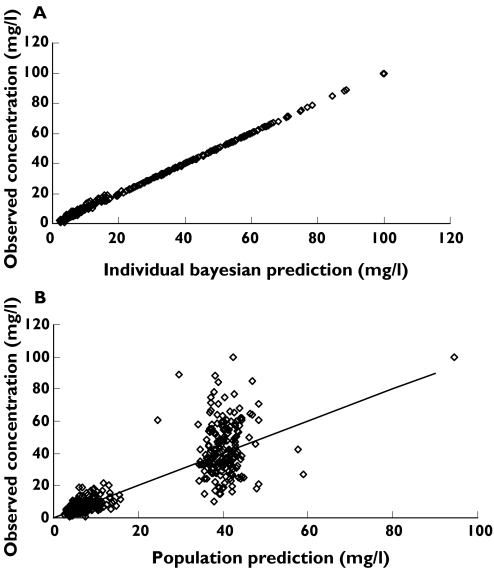
Results: A one-compartment linear disposition model with zero order input (0.3 h i.v. infusion) and first-order elimination was used. The population parameter estimate for volume of distribution (V) was 40.2 l per 70 kg. Clearance (CL) increased from 0.486 l h(-1) per 70 kg at 24 weeks PCA to 0.940 l h(-1) per 70 kg by 30 weeks PCA. The population parameter variability (PPV) for CL and V was 0.336 and 0.451. The use of a NSAID (either aspirin or ibuprofen) in the first day of life reduced amikacin clearance by 22%. Overall 65% of the variability of CL was predictable. Weight explained 48%, PCA 15% and NSAIDs 2%.
Conclusions: Size and post-conception age are the major contributors to clearance variability in extreme premature neonates (<31 weeks PCA). The large (35% of total) unexplained variability in clearance reinforces the need for target concentration intervention to reduce variability in exposure to a safe and effective range.
Figures
Similar articles
-
Vancomycin pharmacokinetics in preterm neonates and the prediction of adult clearance.Br J Clin Pharmacol. 2007 Jan;63(1):75-84. doi: 10.1111/j.1365-2125.2006.02725.x. Epub 2006 Jul 21. Br J Clin Pharmacol. 2007. PMID: 16869817 Free PMC article.
-
Dopamine is not an independent risk factor for reduced amikacin clearance in extremely low-birth-weight infants.Pediatr Crit Care Med. 2006 Mar;7(2):143-6. doi: 10.1097/01.PCC.0000200971.65255.F0. Pediatr Crit Care Med. 2006. PMID: 16446602
-
Impact of ibuprofen administration on renal drug clearance in the first weeks of life.Methods Find Exp Clin Pharmacol. 2006 Oct;28(8):519-22. doi: 10.1358/mf.2006.28.8.1037489. Methods Find Exp Clin Pharmacol. 2006. PMID: 17136231 Clinical Trial.
-
Clinical pharmacokinetics of aminoglycosides in the neonate: a review.Eur J Clin Pharmacol. 2009 Apr;65(4):419-27. doi: 10.1007/s00228-008-0599-y. Epub 2008 Dec 23. Eur J Clin Pharmacol. 2009. PMID: 19104791 Review.
-
The amikacin research program: a stepwise approach to validate dosing regimens in neonates.Expert Opin Drug Metab Toxicol. 2017 Feb;13(2):157-166. doi: 10.1080/17425255.2017.1234606. Epub 2016 Sep 21. Expert Opin Drug Metab Toxicol. 2017. PMID: 27623706 Review.
Cited by
-
Evaluating renal function and age as predictors of amikacin clearance in neonates: model-based analysis and optimal dosing strategies.Br J Clin Pharmacol. 2016 Sep;82(3):793-805. doi: 10.1111/bcp.13016. Epub 2016 Jun 30. Br J Clin Pharmacol. 2016. PMID: 27198625 Free PMC article. Clinical Trial.
-
The role of population PK-PD modelling in paediatric clinical research.Eur J Clin Pharmacol. 2011 May;67 Suppl 1(Suppl 1):5-16. doi: 10.1007/s00228-009-0782-9. Epub 2010 Mar 26. Eur J Clin Pharmacol. 2011. PMID: 20340012 Free PMC article. Review.
-
Cerebrospinal fluid compartmental pharmacokinetics of amikacin in neonates.Antimicrob Agents Chemother. 2008 Jun;52(6):1934-9. doi: 10.1128/AAC.01099-07. Epub 2008 Mar 31. Antimicrob Agents Chemother. 2008. PMID: 18378715 Free PMC article.
-
Interindividual variability of aminoglycoside pharmacokinetics in preterm neonates at birth.Eur J Clin Pharmacol. 2006 Dec;62(12):1011-2. doi: 10.1007/s00228-006-0204-1. Epub 2006 Sep 28. Eur J Clin Pharmacol. 2006. PMID: 17006675 No abstract available.
-
Predictive Performance of Population Pharmacokinetic Models for Amikacin in Term Neonates.Paediatr Drugs. 2023 May;25(3):365-375. doi: 10.1007/s40272-023-00564-z. Epub 2023 Mar 21. Paediatr Drugs. 2023. PMID: 36943583 Free PMC article.
References
-
- Mattie H. The importance of pharmacokinetics and pharmacodynamics for effective treatment of infections. Clin Invest. 1993;71:480–2. - PubMed
-
- Moore RD, Lietman PS, Smith CR. Clinical response to aminoglycoside therapy: importance of the ratio of peak concentration to minimal inhibitory concentration. J Infect Dis. 1987;155:93–9. - PubMed
-
- Langhendries JP, Battisti O, Bertrand JM, Francois A, Kalenga M, Darimont J, Scalais E, Wallemacq P. Adaptation in neonatology of the once-daily concept of aminoglycoside administration: evaluation of a dosing chart for amikacin in an intensive care unit. Biol Neonate. 1998;74:351–62. - PubMed
-
- Langhendries JP, Battisti O, Bertrand JM, Francois A, Darimont J, Ibrahim S, Tulkens PM, Bernard A, Buchet JP, Scalais E. Once-a-day administration of amikacin in neonates: assessment of nephrotoxicity and ototoxicity. Dev Pharmacol Ther. 1993;20:220–30. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
