

Voluntary electronic reporting of medical errors and adverse events. An analysis of 92,547 reports from 26 acute care hospitals
- PMID: 16390502
- PMCID: PMC1484668
- DOI: 10.1111/j.1525-1497.2006.00322.x
Voluntary electronic reporting of medical errors and adverse events. An analysis of 92,547 reports from 26 acute care hospitals
Abstract
Objective: To describe the rate and types of events reported in acute care hospitals using an electronic error reporting system (e-ERS).
Design: Descriptive study of reported events using the same e-ERS between January 1, 2001 and September 30, 2003.
Setting: Twenty-six acute care nonfederal hospitals throughout the U.S. that voluntarily implemented a web-based e-ERS for at least 3 months.
Participants: Hospital employees and staff.
Intervention: A secure, standardized, commercially available web-based reporting system.
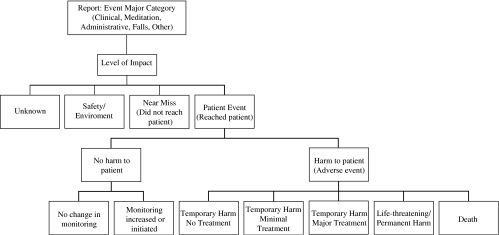
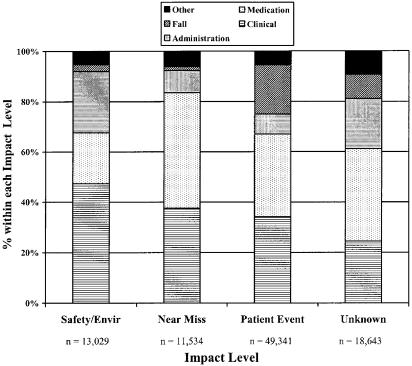
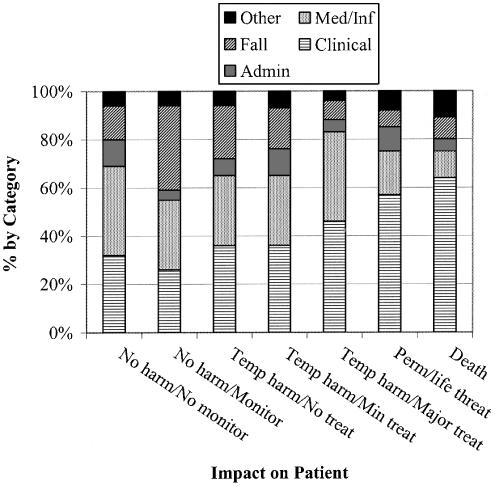
Results: Median duration of e-ERS use was 21 months (range 3 to 33 months). A total of 92,547 reports were obtained during 2,547,154 patient-days. Reporting rates varied widely across hospitals (9 to 95 reports per 1,000 inpatient-days; median=35). Registered nurses provided nearly half of the reports; physicians contributed less than 2%. Thirty-four percent of reports were classified as nonmedication-related clinical events, 33% as medication/infusion related, 13% were falls, 13% as administrative, and 6% other. Among 80% of reports that identified level of impact, 53% were events that reached a patient ("patient events"), 13% were near misses that did not reach the patient, and 14% were hospital environment problems. Among 49,341 patient events, 67% caused no harm, 32% temporary harm, 0.8% life threatening or permanent harm, and 0.4% contributed to patient deaths.
Conclusions: An e-ERS provides an accessible venue for reporting medical errors, adverse events, and near misses. The wide variation in reporting rates among hospitals, and very low reporting rates by physicians, requires investigation.
Figures
References
-
- Kohn LT, Corrigan JM, Donaldson MS, editors. To Err Is Human. Washington, DC: National Academy Press; 1999. - PubMed
-
- Leape LL, Berwick DM, Bates DW. What practices will most improve safety: evidence-based medicine meets patient safety. JAMA. 2002;288:501–7. - PubMed
-
- Bates DW, Cullen DJ, Laird N, et al. Incidence of adverse drug events and potential adverse drug events: implications for prevention. JAMA. 1995;274:29–34. - PubMed
-
- Andrews L, Stocking C, Krizek T, et al. An alternative strategy for studying adverse events in medical care. Lancet. 1997;349:309. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources