

doi: 10.1084/jem.20050390.
Epub 2006 Jan 3.
Identification of the target self-antigens in reperfusion injury
Affiliations
- PMID: 16390934
- PMCID: PMC2118091
- DOI: 10.1084/jem.20050390
Item in Clipboard
Identification of the target self-antigens in reperfusion injury
J Exp Med.
.
Abstract
Reperfusion injury (RI), a potential life-threatening disorder, represents an acute inflammatory response after periods of ischemia resulting from myocardial infarction, stroke, surgery, or trauma. The recent identification of a monoclonal natural IgM that initiates RI led to the identification of nonmuscle myosin heavy chain type II A and C as the self-targets in two different tissues. These results identify a novel pathway in which the innate response to a highly conserved self-antigen expressed as a result of hypoxic stress results in tissue destruction.
Figures
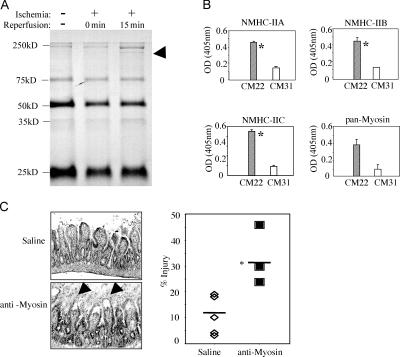
Immune precipitation of ischemia-specific antigens. (A) Detection of a unique band (arrowhead) at ∼250 kD on SDS-PAGE (8%). Size markers are indicated on the left. Intestinal lysates were prepared from RAG-1−/− mice reconstituted with IgM CM-22 and either sham control (no ischemia) or subjected to ischemia, followed by reperfusion for 0 or 15 min. (B) In vitro binding of IgM CM-22 to NMHC-II. ELISA plates were coated with rabbit IgG antibodies specific for each of the three different isoforms of NMHC-II (top left, isoform A; top right, isoform B; bottom left, isoform C; or bottom right, anti–pan-myosin antibody). Bound myosin HC from intestinal lysates was detected by IgM CM-22 or CM-31. Results represent means ± SEM of OD 405 nm units and are representative of triplicate samples. (C) Anti–pan-myosin antibody restores RI in ischemic RAG-1−/− mice. RAG-1−/− mice were injected i.v. with saline (top left) or 50 μg of rabbit IgG anti–pan-myosin (bottom left), followed by RI treatment. (right) Scatter plot of pathology scores in which each symbol represents a single animal. *, P < 0.05.
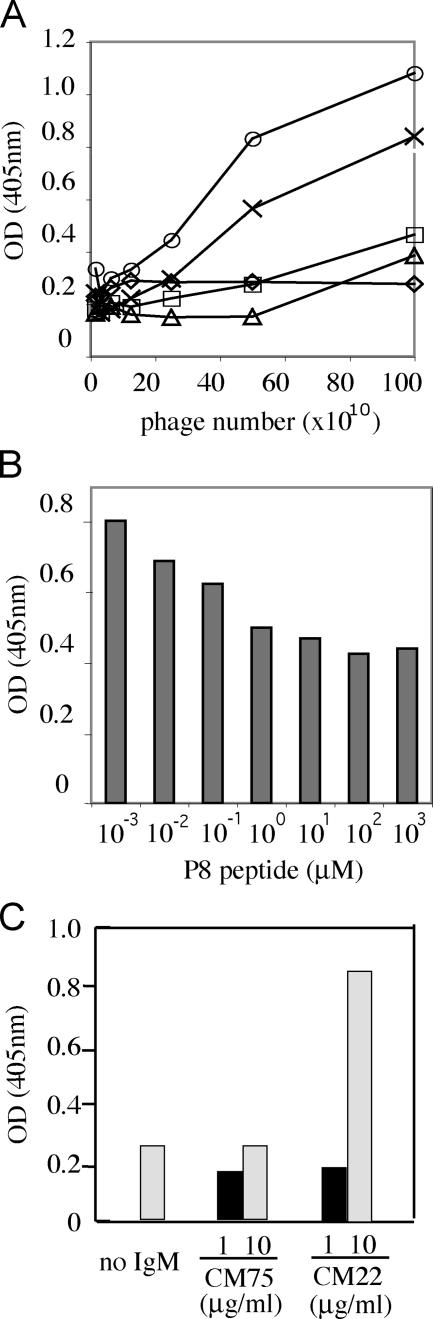
Screening of M13 phage display library identifies IgM CM-22–specific peptides. (A) ELISA comparison of four phage clones isolated from an enriched pool IgM CM-22–selected phage. Phage clone P8 binds with the highest relative efficiency (▵, P1 clone; ×, P5 clone; □, P7 clone; ○, P8 clone; and ⋄, control M13). Plate was coated with a solution of IgM CM-22 before addition of varying concentrations of phage clones. (B) Synthetic peptide P8 inhibits IgM CM-22 binding of phage clone P8. ELISA was performed with varying concentrations of synthetic P8 peptide added to an IgM CM-22–coated plate before the addition of 5 × 1011 PFU phage. (C) ELISA assay for specific binding of P8 peptide to IgM CM-22. Synthetic P8 peptide was coated on an ELISA plate followed by addition of saline, IgM CM-75, or IgM CM-22 at 1 (closed bar) or 10 (shaded bar) μg/ml. The bound IgM was detected by anti–mouse IgM-AP as described in Materials and methods. Results in A–C are representative of at least three independent experiments.
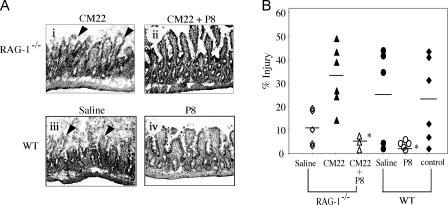
P8 peptide blocks RI in RAG-1−/− mice and WT animals. (A, i and ii) Representative sections (stained with hematoxylin and eosin) prepared after RI treatment in RAG-1−/− mice with IgM CM-22 alone or mixed with P8 peptide, respectively. (iii and iv) Representative sections prepared from WT mice and treated for intestinal RI that received either saline or P8 peptide 5 min before reperfusion. Arrowheads indicate pathologic features of injury. Magnification, 200. (B) Scatter plot indicates mean pathology score of each group of treated animals. Each symbol represents one animal. Control group is WT mice pretreated with a control peptide (AGCMPYVRIPTA) at a similar dose of P8 peptide. *, P < 0.05 as determined by Student's t test of the P8 treated versus untreated groups.

SPR. (A) Binding isotherms for samples of the N2 peptide with concentrations from 10.5 to 120 μM injected over the IgM CM-22–coupled surface. (B) Binding isotherm for a same-length random sequence control peptide (AGCMPYVRIPTA) injected at a concentration of 117 μM over the IgM CM-22–coupled surfaces. (C) Nonlinear curve fitting with a 1:1 Langmuir binding isotherm to the steady-state response levels for the injection showed in A (χ2 = 10). (D) The binding isotherm for the injection of the N2 peptide at 120 μM over a surface coupled with control IgM CM-31. In A, B, and D, the injection phases had a duration of 240 s each, with the ends of the injection marked by arrows.

Treatment of mice with NMHC-II N2 peptide blocks intestinal RI. (A) Representative sections prepared from WT mice treated for intestinal RI and injected i.v. with either saline (i) or 40 μM N2 peptide (ii) 5 min before reperfusion. (B) Scatter plot indicates mean pathology score of each group of treated animals. WT mice were injected with saline or varying concentrations (final serum concentrations of N2 are indicated) of N2 peptide 5 min before reperfusion. Each symbol represents a single mouse. *, P < 0.05 as determined by Student's t test. (C) Scatter plot indicates mean plasma levels of 40-kD HRP of each group of treated animals 3 h after reperfusion. WT mice were administered HRP by gavage 10 min before the induction of intestinal RI and further treated with control, saline, or 40 μM N2 peptide 5 min before reperfusion. Each symbol represents a single mouse. *, P < 0.05, based on Student's t test. (D) 32 and 40 μM N2 peptide blocks IgM binding and activation of complement in intestinal RI. Representative cryosections of intestinal tissues were harvested after intestinal RI and treated with antibodies specific for mouse IgM, C4, or C3. Magnification, 400. Results are representative of at least five experiments. Immunohistology was not performed on tissues harvested from mice treated with the lower doses of peptide. WT mice were without N2 (i–iv) or pretreated with N2 (v–viii). (i, iii, v, and vii) Sections were stained with anti-IgM–biotin, followed by streptavidin–Alexa 568 (red), and counterstained with DAPI (violet). Sections in panels ii and vi were stained with anti-C4–FITC (green), and the sections in panels iv and viii were stained with anti-C3–FITC (green).

N2 peptide blocks vascular leak in intestinal RI. (A, i–iii) Representative images of microvilli within the jejuneum of sham, saline, or N2 administered mice, respectively. Mice were treated for RI as described in Fig. 5, except that 5 min before reperfusion the later two groups were injected i.v. with a mixture of vascular probe (AngioSense 680, red) and Rhodamine 6G (green) in saline or N2 peptide (40 μM final concentration). (i) Results of the sham group identify microvasculature of individual microvilli in which red indicates blood vessels and green outlines enterocytes and lamina propria. (ii) Saline group images indicate extensive leakage of the vascular probe into lamina propria and surrounding tissues. (iii) N2 peptide group results indicate relatively normal vasculature within microvilli and limited leakage of vascular probe. (B) Scatter plot of ratio of intensity of signal of vessels (V) versus background (B). The horizontal lines indicate the mean of samples analyzed. Each symbol indicates a representative measurement from representative images of at least three mice per group, and means ± SD were calculated. *, P < 0.001, as determined by Student's t test.
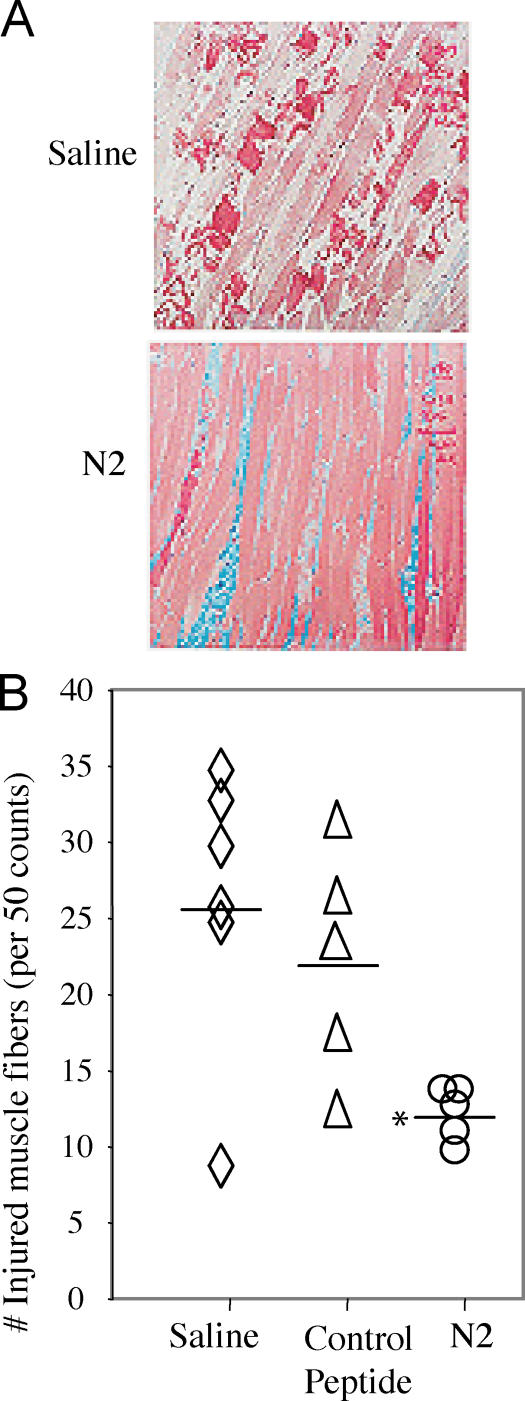
N2 peptide is protective in skeletal muscle model of RI. WT mice were treated in the hindlimb model of RI and administered either saline, control, or N2 peptide before reperfusion. (A) Representative sections of hindlimb muscle isolated from mice pretreated with either saline (top) or 40 μM N2 peptide (bottom). Samples were stained with Masson's Trichrome for histology. Magnification, 200. (B) Injury score based on the percentage of injured fibers per 50 counted. Each symbol represents a single mouse. *, P < 0.05 as determined by Student's t test between N2 and control peptide; P < 0.01 as determined by Student's t test between N2 and saline; and P < 0.05 as determined by ANOVA for all groups.
References
-
- Wu, B., A. Ootani, R. Iwakiri, T. Fujise, S. Tsunada, S. Toda, and K. Fujimoto. 2004. Ischemic preconditioning attenuates ischemia-reperfusion-induced mucosal apoptosis by inhibiting the mitochondria-dependent pathway in rat small intestine. Am. J. Physiol. Gastrointest. Liver Physiol. 286:G580–G587. - PubMed
-
- Szabo, G., L. Liaudet, S. Hagl, and C. Szabo. 2004. Poly(ADP-ribose) polymerase activation in the reperfused myocardium. Cardiovasc. Res. 61:471–480. - PubMed
-
- Becker, L.B. 2004. New concepts in reactive oxygen species and cardiovascular reperfusion physiology. Cardiovasc. Res. 61:461–470. - PubMed
-
- Becker, L.B., T.L. Vanden Hoek, Z.H. Shao, C.Q. Li, and P.T. Schumacker. 1999. Generation of superoxide in cardiomyocytes during ischemia before reperfusion. Am. J. Physiol. 277:H2240–H2246. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
