

Obstetric factors associated with levator ani muscle injury after vaginal birth
- PMID: 16394052
- PMCID: PMC2841321
- DOI: 10.1097/01.AOG.0000194063.63206.1c
Obstetric factors associated with levator ani muscle injury after vaginal birth
Abstract
Objective: To identify obstetric factors associated with development of levator ani injury after vaginal birth.
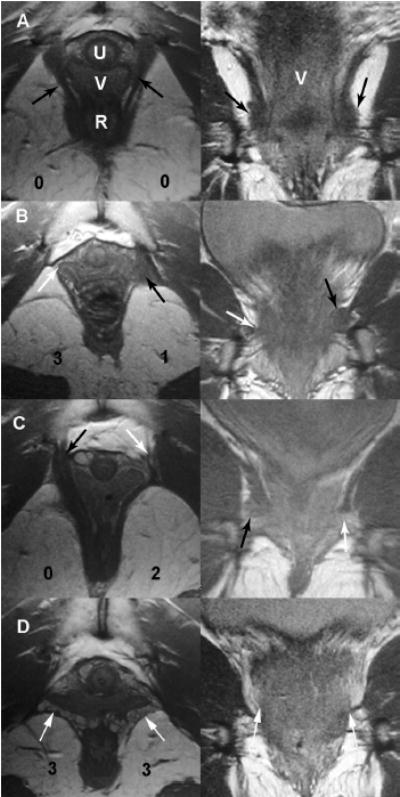
Methods: Magnetic resonance images were taken of the pelvic floor of 160 women 9 to 12 months after first term vaginal delivery. Half the women had de novo stress incontinence and half were continent controls. Abnormalities of the pubovisceral portion were identified on magnetic resonance as present or absent. Defect severity was further scored in each muscle from 0 (no defect) to 3 (complete muscle loss). A summed score for the 2 sides (0 to 6) was assigned and grouped as minor (0-3) or major (4-6). Obstetric details were collected. The association between obstetric variables and muscle injury were analyzed using Fisher exact test and t tests.
Results: The following increased odds ratios for levator defect were found: forceps use 14.7 (95% confidence interval [CI] 4.9-44.3), anal sphincter rupture 8.1 (95% CI 3.3-19.5) and episiotomy 3.1 (95% CI 1.4-7.2) but not vacuum delivery 0.9 (95% CI 0.19-4.3), epidural use 0.9 (95% CI 0.4-2.0), or oxytocin use 0.8 (95% CI 0.3-1.8). Women with levator injury were 3.5 years older and had a 78-minute longer second stage of labor. Differences in gestational age, birth weight, and head circumference were not statistically significant. A major defect in the pubovisceral muscle was seen in 22 women and a minor defect in 7 women.
Conclusion: Injuries to the levator ani muscles in women after their first vaginal delivery are associated with several obstetric factors indicating difficult vaginal birth and with older age.
Level of evidence: II-3.
Figures
References
-
- Mant J, Painter R, Vessey M. Epidemiology of genital prolapse: observations from the Oxford Family Planning Association Study. Br J Obstet Gynaecol. 1997;104:579–85. - PubMed
-
- Rortveit G, Hannestad YS, Daltveit AK, Hunskaar S. Age- and type-dependent effects of parity on urinary incontinence: the Norwegian EPINCONT study. Obstet Gynecol. 2001;98:1004–10. - PubMed
-
- Kirschner-Hermanns R, Wein B, Niehaus S, Schaefer W, Jakse G. The contribution of magnetic resonance imaging of the pelvic floor to the understanding of urinary incontinence. Br J Urol. 1993;72:715–8. - PubMed
-
- Tunn R, Paris S, Fischer W, Hamm B, Kuchinke J. Static magnetic resonance imaging of the pelvic floor muscle morphology in women with stress urinary incontinence and pelvic prolapse. Neurourol Urodyn. 1998;17:579–89. - PubMed
-
- Hoyte L, Schierlitz L, Zou K, Flesh G, Fielding J. Two- and 3-dimensional MRI comparison of levator ani structure, volume, and integrity in women with stress incontinence and prolapse. Am J Obstet Gynecol. 2001;185:11–9. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
