

Review
doi: 10.1016/j.hrthm.2005.09.021.
Neural modulation of cardiac arrhythmias and sudden cardiac death
Affiliations
- PMID: 16399065
- PMCID: PMC2566299
- DOI: 10.1016/j.hrthm.2005.09.021
Item in Clipboard
Review
Neural modulation of cardiac arrhythmias and sudden cardiac death
Heart Rhythm.
2006 Jan.
No abstract available
Figures

Schematic illustration of intracellular Ca2+ cycling and associated second messenger pathways in cardiomyocytes (figure modified from Yano et al. J. Clin. Invest. 2005;115:556–564). AC, adenylyl cyclase; α, G protein subunit α; α-receptor, α-adrenergic receptor; β, G protein subunit β; β-receptor, β-adrenergic receptor; γ, G protein subunit γ, LTCC, L-type Ca2+ channel; CaMKII, Ca2+-calmodulin kinase II; I-1, inhibitor 1; NCX, Na+/Ca2+ exchanger; P, phosphate group; PLC, phosphatase 2A; ATP, SR Ca2+-ATPAse. Reproduced with permission from ref .

Proposed scheme of events leading to DADs and triggered tachyarrhythmia. (A) Congenital (e.g., ankyrin-B mutation) and/or acquired factors (e.g., ischemia, hypertrophy, increased sympathetic tone) will cause a diastolic Ca2+ leak through RyR2, resulting in localized and transient increases in [Ca2+], in cardiomyocytes. (B) Representative series of images showing changes in [Ca2+], during a Ca2+ wave in a single cardiomyocyte loaded with a Ca2+-sensitive fluorescent dye. Images were obtained at 117-ms intervals. Focally elevated Ca2+ (ii) diffuses to adjacent junctional SR, where it initiates more Ca2+ release events, resulting in a propagating Ca2+ wave (iii–vii). Reproduced with permission from Subramanian et al Biophysical Journal 2001; 80:1–11. (C) The Ca2+ wave through activation of Ca2+-sensitive inward currents will depolarize the cardiomyocytes (DAD). In cardiomyocytes the inward INa/Ca is the major candidate for the transient inward current underlying DADs, although the role of the Ca2+-activated CI-current [ICl(Ca)] and a Ca2+-sensitive nonspecific cation current [INS (Ca)] cannot be excluded. If of sufficient magnitude, the DAD will depolarize the cardiomyocyte above threshold resulting in a single or repetitive premature heartbeat (red arrows), which can trigger an arrhythmia. Modified with permission from Circulation Research and Nature. Downregulation of the inward rectifier potassium current (IK1), upregulation of INa/Ca, or a slight increase in intercellular electrical resistance can promote the generation of DAD-triggered action potentials. S, stimulus. Reproduced with permission from ref .

Proposed scheme of events leading to DADs and triggered tachyarrhythmia. (A) Congenital (e.g., ankyrin-B mutation) and/or acquired factors (e.g., ischemia, hypertrophy, increased sympathetic tone) will cause a diastolic Ca2+ leak through RyR2, resulting in localized and transient increases in [Ca2+], in cardiomyocytes. (B) Representative series of images showing changes in [Ca2+], during a Ca2+ wave in a single cardiomyocyte loaded with a Ca2+-sensitive fluorescent dye. Images were obtained at 117-ms intervals. Focally elevated Ca2+ (ii) diffuses to adjacent junctional SR, where it initiates more Ca2+ release events, resulting in a propagating Ca2+ wave (iii–vii). Reproduced with permission from Subramanian et al Biophysical Journal 2001; 80:1–11. (C) The Ca2+ wave through activation of Ca2+-sensitive inward currents will depolarize the cardiomyocytes (DAD). In cardiomyocytes the inward INa/Ca is the major candidate for the transient inward current underlying DADs, although the role of the Ca2+-activated CI-current [ICl(Ca)] and a Ca2+-sensitive nonspecific cation current [INS (Ca)] cannot be excluded. If of sufficient magnitude, the DAD will depolarize the cardiomyocyte above threshold resulting in a single or repetitive premature heartbeat (red arrows), which can trigger an arrhythmia. Modified with permission from Circulation Research and Nature. Downregulation of the inward rectifier potassium current (IK1), upregulation of INa/Ca, or a slight increase in intercellular electrical resistance can promote the generation of DAD-triggered action potentials. S, stimulus. Reproduced with permission from ref .

Proposed scheme of events leading to DADs and triggered tachyarrhythmia. (A) Congenital (e.g., ankyrin-B mutation) and/or acquired factors (e.g., ischemia, hypertrophy, increased sympathetic tone) will cause a diastolic Ca2+ leak through RyR2, resulting in localized and transient increases in [Ca2+], in cardiomyocytes. (B) Representative series of images showing changes in [Ca2+], during a Ca2+ wave in a single cardiomyocyte loaded with a Ca2+-sensitive fluorescent dye. Images were obtained at 117-ms intervals. Focally elevated Ca2+ (ii) diffuses to adjacent junctional SR, where it initiates more Ca2+ release events, resulting in a propagating Ca2+ wave (iii–vii). Reproduced with permission from Subramanian et al Biophysical Journal 2001; 80:1–11. (C) The Ca2+ wave through activation of Ca2+-sensitive inward currents will depolarize the cardiomyocytes (DAD). In cardiomyocytes the inward INa/Ca is the major candidate for the transient inward current underlying DADs, although the role of the Ca2+-activated CI-current [ICl(Ca)] and a Ca2+-sensitive nonspecific cation current [INS (Ca)] cannot be excluded. If of sufficient magnitude, the DAD will depolarize the cardiomyocyte above threshold resulting in a single or repetitive premature heartbeat (red arrows), which can trigger an arrhythmia. Modified with permission from Circulation Research and Nature. Downregulation of the inward rectifier potassium current (IK1), upregulation of INa/Ca, or a slight increase in intercellular electrical resistance can promote the generation of DAD-triggered action potentials. S, stimulus. Reproduced with permission from ref .
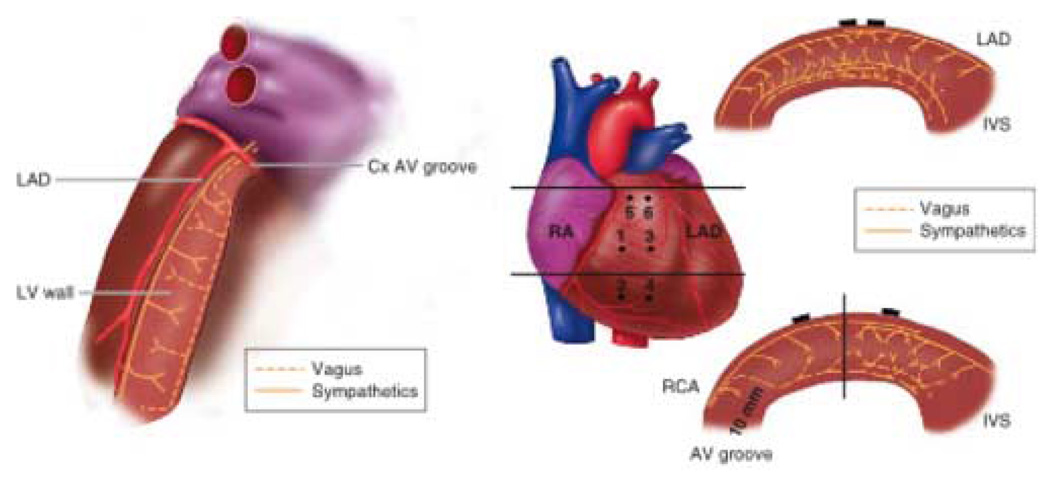
Intraventricular role of sympathetic and vagal nerves to the left and right ventricles. Left. Schematic of the transverse view of the left ventricle (LV) showing functional pathways of the efferent and afferent sympathetic and vagal nerves. Right. Schematic of the transverse views of the right ventricular (RV) wall showing functional pathways of the efferent sympathetic and vagal nerves. Top right. Transverse view of the RV outflow tract at the upper horizontal line on the heart image (middle panel). Bottom right. Transverse view of the anterolateral wall at the lower horizontal line on the heart image (middle panel). The vertical solid line indicates the center of the RV anterolateral wall. Closed circles indicate position of plunge electrodes labeled 1 to 6. Cx= circumflex coronary artery; IVS = interventricular septum; LAD = left anterior descending coronary artery; RA = right atrium; RCA = right coronary artery. (Reproduced with permission from Ito M, Zipes DP Circulation 1994; 90:1459)

Factors contributing to arrhythmogenesis in hearts with heterogeneous sympathetic innervation. Myocardial injury (e.g., myocardial infarction) or chronic hypercholesterolemia will cause a spatially uneven increase in sympathetic neurotransmitters. Chronic, nonuniform elevations of neurotransmitters, through alterations in the expression of L-type Ca2+ channels and K+ channels, create spatial dispersion of action potential duration. Action potential prolongation and augmented Ca2+ influx through L-type Ca2+ channels combined to increase the susceptibility to EAD-and/ or DAD-triggered activity in hyperinnervated regions. If the triggered beat propagates throughout the rest of the heart, the preexisting spatial dispersion of action potential duration and, thus, myocardial refractoriness facilitate the initial of tachyarrhythmias. Locally elevated levels of neuropeptide Y and norepinephrine may increase coronary artery tone, thereby critically reducing the coronary perfusion reserve under condition of increased oxygen demand (e.g., physical and/or emotional stress) and causing regional ischemia, which contribute to the development of an arrhythmia. Reproduced with permission from ref .
References
-
- Tomaselli GF, Zipes DP. What causes sudden death in heart failure? Circ Res. 2004 Oct 15;95(8):754–763. - PubMed
-
- Rubart M, Zipes DP. Genes and cardiac repolarization: the challenge ahead. Circulation. 2005 Aug 30;112(9):1242–1244. - PubMed
-
- Priori S, Zipes DP. Sudden Cardiac Death. Elsevier Pub; 2006.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
