

Profit and loss analysis for an intensive care unit (ICU) in Japan: a tool for strategic management
- PMID: 16403235
- PMCID: PMC1395358
- DOI: 10.1186/1472-6963-6-1
Profit and loss analysis for an intensive care unit (ICU) in Japan: a tool for strategic management
Abstract
Background: Accurate cost estimate and a profit and loss analysis are necessary for health care practice. We performed an actual financial analysis for an intensive care unit (ICU) of a university hospital in Japan, and tried to discuss the health care policy and resource allocation decisions that have an impact on critical intensive care.
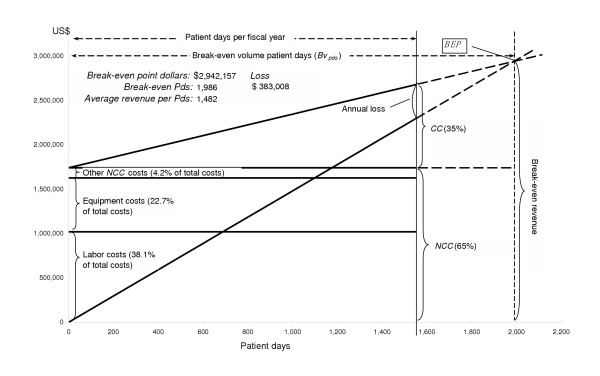
Methods: The costs were estimated by a department level activity based costing method, and the profit and loss analysis was based on a break-even point analysis. The data used included the monthly number of patients, the revenue, and the direct and indirect costs of the ICU in 2003.
Results: The results of this analysis showed that the total costs of USD 2,678,052 of the ICU were mainly incurred due to direct costs of 88.8%. On the other hand, the actual annual total patient days in the ICU were 1,549 which resulted in revenues of USD 2,295,044. However, it was determined that the ICU required at least 1,986 patient days within one fiscal year based on a break-even point analysis. As a result, an annual deficit of USD 383,008 has occurred in the ICU.
Conclusion: These methods are useful for determining the profits or losses for the ICU practice, and how to evaluate and to improve it. In this study, the results indicate that most ICUs in Japanese hospitals may not be profitable at the present time. As a result, in order to increase the income to make up for this deficit, an increase of 437 patient days in the ICU in one fiscal year is needed, and the number of patients admitted to the ICU should thus be increased without increasing the number of beds or staff members. Increasing the number of patients referred from cooperating hospitals and clinics therefore appears to be the best strategy for achieving these goals.
Figures
References
-
- Report from the Second American Thoracic Society Workshop on Outcomes Research Understanding Costs and Cost-Effectiveness in Critical Care. Am J Respir Crit Care Med. 2002;165:540–550. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
