

Nosocomial pneumonia : rationalizing the approach to empirical therapy
- PMID: 16409013
- PMCID: PMC7100095
- DOI: 10.2165/00151829-200605010-00002
Nosocomial pneumonia : rationalizing the approach to empirical therapy
Abstract
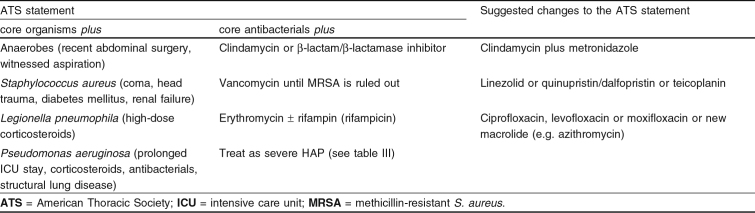
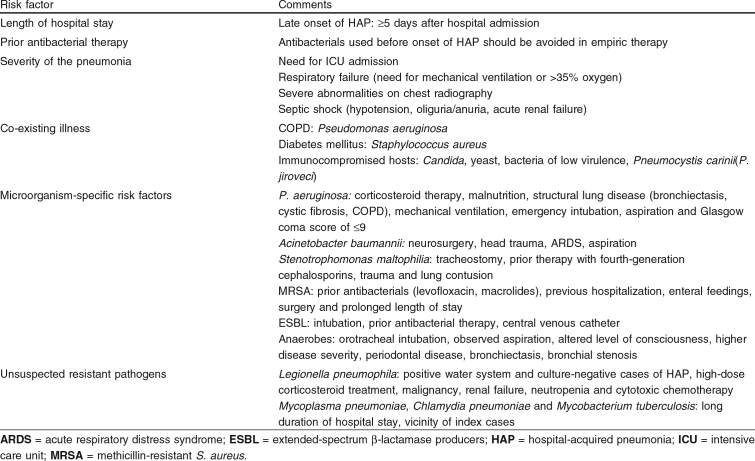
Nosocomial pneumonia or hospital-acquired pneumonia (HAP) causes considerable morbidity and mortality. It is the second most common nosocomial infection and the leading cause of death from hospital-acquired infections. In 1996 the American Thoracic Society (ATS) published guidelines for empirical therapy of HAP. This review focuses on the literature that has appeared since the ATS statement. Early diagnosis of HAP and its etiology is crucial in guiding empirical therapy. Since 1996, it has become clear that differentiating mere colonization from etiologic pathogens infecting the lower respiratory tract is best achieved by employing bronchoalveolar lavage (BAL) or protected specimen brush (PSB) in combination with quantitative culture and detection of intracellular microorganisms. Endotracheal aspirate and non-bronchoscopic BAL/PSB in combination with quantitative culture provide a good alternative in patients suspected of ventilator-associated pneumonia. Since culture results take 2-3 days, initial therapy of HAP is by definition empirical. Epidemiologic studies have identified the most frequently involved pathogens: Enterobacteriaceae, Haemophilus influenzae, Streptococcus pneumoniae and Staphylococcus aureus ('core pathogens'). Empirical therapy covering only the 'core pathogens' will suffice in patients without risk factors for resistant microorganisms. Studies that have appeared since the ATS statement issued in 1996, demonstrate several new risk factors for HAP with multiresistant pathogens. In patients with risk factors, empirical therapy should consist of antibacterials with a broader spectrum. The most important risk factors for resistant microorganisms are late onset of HAP (>/=5 days after admission), recent use of antibacterial therapy, and mechanical ventilation. Multiresistant bacteria of specific interest are methicillin-resistant S. aureus (MRSA), Pseudomonas aeruginosa, Acinetobacter calcoaceticus-baumannii, Stenotrophomonas maltophilia and extended-spectrum beta-lactamase (ESBL)-producing Enterobacteriaceae. Each of these organisms has its specific susceptibility pattern, demanding appropriate antibacterial treatment. To further improve outcomes, specific therapeutic options for multiresistant pathogens and pharmacological factors are discussed. Antibacterials developed since 1996 or antibacterials with renewed interest (linezolid, quinupristin/dalfopristin, teicoplanin, meropenem, new fluoroquinolones, and fourth-generation cephalosporins) are discussed in the light of developing resistance.Since the ATS statement, many reports have shown increasing incidences of resistant microorganisms. Therefore, one of the most important conclusions from this review is that empirical therapy for HAP should not be based on general guidelines alone, but that local epidemiology should be taken into account and used in the formulation of local guidelines.
Figures


Similar articles
-
Sulopenem: An Intravenous and Oral Penem for the Treatment of Urinary Tract Infections Due to Multidrug-Resistant Bacteria.Drugs. 2022 Apr;82(5):533-557. doi: 10.1007/s40265-022-01688-1. Epub 2022 Mar 16. Drugs. 2022. PMID: 35294769 Review.
-
[Guidelines for treatment of pneumonia in intensive care units].Infez Med. 2005;Suppl:7-17. Infez Med. 2005. PMID: 16801748 Review. Italian.
-
Hospital-acquired pneumonia and ventilator-associated pneumonia in adults at Siriraj Hospital: etiology, clinical outcomes, and impact of antimicrobial resistance.J Med Assoc Thai. 2010 Jan;93 Suppl 1:S126-38. J Med Assoc Thai. 2010. PMID: 20364567
-
[Analysis of pathogen spectrum and antimicrobial resistance of pathogens associated with hospital-acquired infections collected from 11 teaching hospitals in 2018].Zhonghua Yi Xue Za Zhi. 2020 Dec 22;100(47):3775-3783. doi: 10.3760/cma.j.cn112137-20200430-01389. Zhonghua Yi Xue Za Zhi. 2020. PMID: 33379842 Chinese.
-
[Analysis of pathogen spectrum and resistance of clinical common organisms causing bloodstream infections, hospital-acquired pneumonia and intra-abdominal infections from thirteen teaching hospitals in 2013].Zhonghua Yi Xue Za Zhi. 2015 Jun 9;95(22):1739-46. Zhonghua Yi Xue Za Zhi. 2015. PMID: 26704158 Chinese.
Cited by
-
Detection of Eight Respiratory Bacterial Pathogens Based on Multiplex Real-Time PCR with Fluorescence Melting Curve Analysis.Can J Infect Dis Med Microbiol. 2020 Feb 26;2020:2697230. doi: 10.1155/2020/2697230. eCollection 2020. Can J Infect Dis Med Microbiol. 2020. PMID: 32184908 Free PMC article.
-
In vitro activity of ceftaroline against Streptococcus pneumoniae isolates exhibiting resistance to penicillin, amoxicillin, and cefotaxime.Antimicrob Agents Chemother. 2008 Nov;52(11):4209-10. doi: 10.1128/AAC.00712-08. Epub 2008 Aug 25. Antimicrob Agents Chemother. 2008. PMID: 18725443 Free PMC article. No abstract available.
-
A Case of Daptomycin-Induced Eosinophilic Pneumonia and Its Management Insights.Cureus. 2025 Apr 29;17(4):e83195. doi: 10.7759/cureus.83195. eCollection 2025 Apr. Cureus. 2025. PMID: 40443582 Free PMC article.
-
Comparison of clinical outcomes in critically ill COVID-19 patients on mechanical ventilation with nosocomial pneumonia between Alpha and Omicron variants.Ther Adv Respir Dis. 2023 Jan-Dec;17:17534666231213642. doi: 10.1177/17534666231213642. Ther Adv Respir Dis. 2023. PMID: 38018405 Free PMC article.
References
-
- Gross PA. Epidemiology of hospital-acquired pneumonia. Semin Respir Infect. 1987;2(1):2–7. - PubMed
-
- George DL. Epidemiology of nosocomial ventilator-associated pneumonia. Infect Control Hosp Epidemiol. 1993;14(3):163–9. - PubMed
-
- Kollef MH. Epidemiology and risk factors for nosocomial pneumonia: emphasis on prevention. Clin Chest Med. 1999;20(3):653–70. - PubMed
-
- Am J Respir Crit Care Med. 1996. - PubMed
-
- Greenaway CA, Embil J, Orr PH, et al. Nosocomial pneumonia on general medical and surgical wards in a tertiary-care hospital. Infect Control Hosp Epidemiol. 1997;18(11):749–56. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical