

Do patients with older-onset rheumatoid arthritis receive less aggressive treatment?
- PMID: 16414968
- PMCID: PMC1798297
- DOI: 10.1136/ard.2005.051144
Do patients with older-onset rheumatoid arthritis receive less aggressive treatment?
Abstract
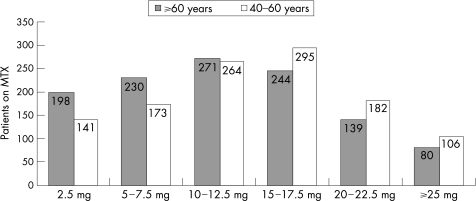
Rheumatoid arthritis among elderly people is an increasingly important health concern. Despite several cross-sectional studies, it has not been clearly established whether there are important clinical differences between elderly-onset rheumatoid arthritis (EORA) and younger-onset rheumatoid arthritis (YORA). The aim of this study was to compare disease activity and treatment in EORA and YORA, using the Consortium of Rheumatology Researchers of North America (CORRONA) registry, a database generated by rheumatologist investigators across the USA. From the CORRONA registry database of 9381 patients with rheumatoid arthritis, 2101 patients with disease onset after the age of 60 years (EORA) were matched, on the basis of disease duration, with 2101 patients with disease onset between the ages of 40 and 60 years (YORA). The primary outcome measures were the proportion of patients on methotrexate, multiple disease-modifying antirheumatic drugs (DMARD) and biological agents (etanercept, infliximab, adalimumab and kineret) in each group. Disease activity and severity differed slightly between the EORA and YORA groups: Disability Index of the Health Assessment Questionnaire: 0.30 v 0.35; tender joint count: 3.7 v 4.7; swollen joint count: 5.3 v 5.2; Disease Activity Score 28: 3.8 v 3.6; patient global assessment: 29.1 v 30.9; physician global assessment: 24.9 v 26.3; patient pain assessment: 31.4 v 34.9. Regarding treatment, the use of methotrexate use was slightly more common among patients with EORA (63.9%) than among those with YORA (59.6%), although the mean methotrexate dose among the YORA group was higher than that in the EORA group. The percentage of patients with EORA who were on multiple DMARD treatment (30.9%) or on biological agents (25%) was considerably lower than that of patients with YORA (40.5% and 33.1%, respectively; p<0.0001). Toxicity related to treatment was very minimal in both groups, whereas toxicities related to methotrexate were more common in the YORA group. Patients with EORA receive biological treatment and combination DMARD treatment less frequently than those with YORA, despite identical disease duration and comparable disease severity and activity.
Conflict of interest statement
Competing interests: None declared.
References
-
- Kerr L D. Inflammatory arthropathy: a review of rheumatoid arthritis in older patients. Geriatrics 20045932–35. - PubMed
-
- van Schaardenburg D, Breedweld F C. Elderly‐onset rheumatoid arthritis. Semin Arthritis Rheum 199423367–378. - PubMed
-
- Kavanaugh A F. Rheumatoid arthritis in the elderly: is it a different disease? Am J Med 199710340S–418. - PubMed
-
- Pincus T, Marcum S B, Callahan L F, Adams R F, Barber J, Barth W F.et al Long term drug therapy for rheumatoid arthritis in seven rheumatology private practices. Second line drugs and prednisone. J Rheumatol 1992191885–1894. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
