

Inequalities in access to medical care by income in developed countries
- PMID: 16415462
- PMCID: PMC1329455
- DOI: 10.1503/cmaj.050584
Inequalities in access to medical care by income in developed countries
Abstract
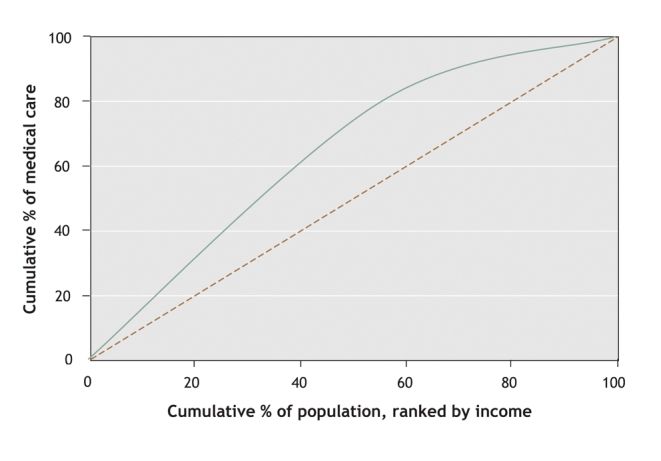
Background: Most of the member countries of the Organization for Economic Cooperation and Development (OECD) aim to ensure equitable access to health care. This is often interpreted as requiring that care be available on the basis of need and not willingness or ability to pay. We sought to examine equity in physician utilization in 21 OECD countries for the year 2000.
Methods: Using data from national surveys or from the European Community Household Panel, we extracted the number of visits to a general practitioner or medical specialist over the previous 12 months. Visits were standardized for need differences using age, sex and reported health levels as proxies. We measured inequity in doctor utilization by income using concentration indices of the need-standardized use.
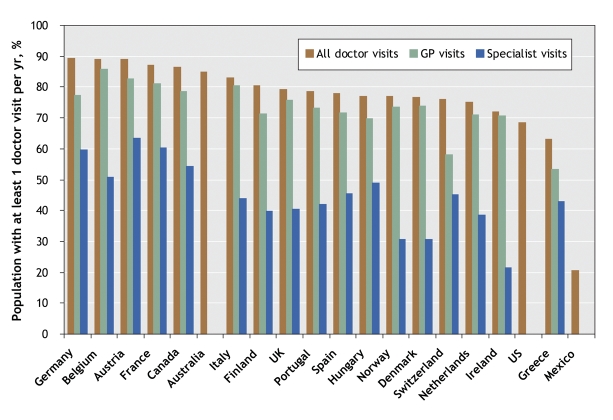
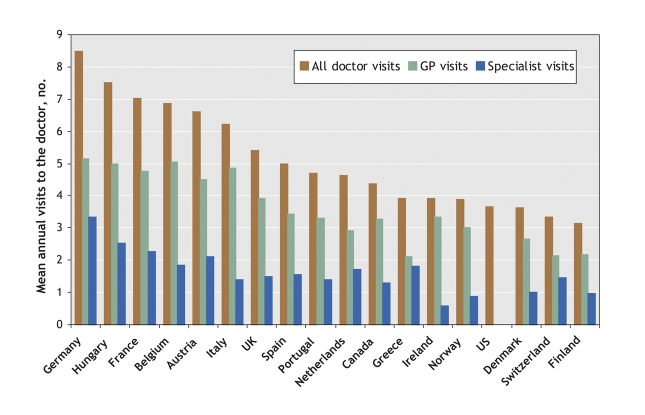
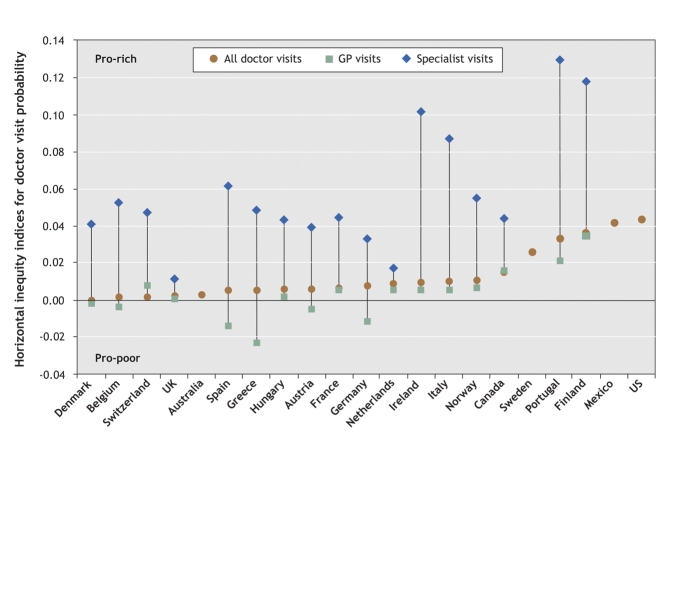
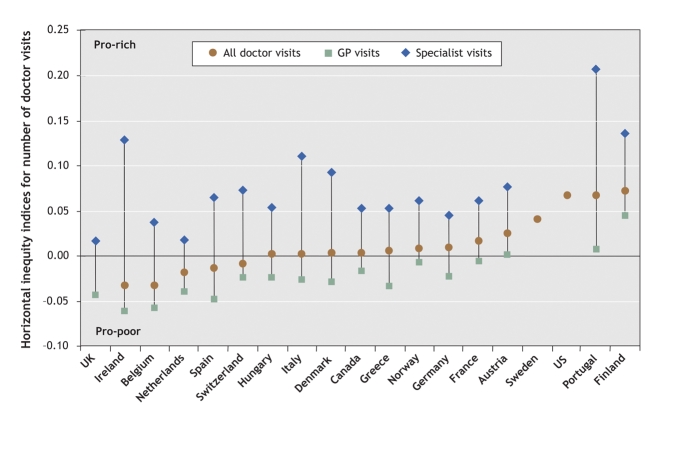
Results: We found inequity in physician utilization favouring patients who are better off in about half of the OECD countries studied. The degree of pro-rich inequity in doctor use is highest in the United States and Mexico, followed by Finland, Portugal and Sweden. In most countries, we found no evidence of inequity in the distribution of general practitioner visits across income groups, and where it does occur, it often indicates a pro-poor distribution. However, in all countries for which data are available, after controlling for need differences, people with higher incomes are significantly more likely to see a specialist than people with lower incomes and, in most countries, also more frequently. Pro-rich inequity is especially large in Portugal, Finland and Ireland.
Interpretation: Although in most OECD countries general practitioner care is distributed fairly equally and is often even pro-poor, the very pro-rich distribution of specialist care tends to make total doctor utilization somewhat pro-rich. This phenomenon appears to be universal, but it is reinforced when private insurance or private care options are offered.
Figures
Comment in
-
Income and equity of access to physician services.CMAJ. 2006 Jan 17;174(2):187-8. doi: 10.1503/cmaj.051214. CMAJ. 2006. PMID: 16415464 Free PMC article. No abstract available.
-
The rate of joint replacement in osteoarthritis depends on the patient's socioeconomic status.Acta Orthop. 2016 Jun;87(3):245-51. doi: 10.3109/17453674.2016.1161451. Epub 2016 Mar 16. Acta Orthop. 2016. PMID: 26982799 Free PMC article.
References
-
- Hurst JW. Performance measurement and improvement in OECD health systems: overview of issues and challenges. In: Measuring up: improving health system performance in OECD countries. Paris: OECD; 2002.
-
- Van Doorslaer E, Masseria C; OECD Health Equity Research Group. Income-related inequality in the use of medical care in 21 OECD countries. In: Towards high-performing health systems: policy studies. Paris: OECD; 2004. p. 109-66.
-
- Docteur E, Oxley H. Health system reform: lessons from experience. In: Towards high-performing health systems: policy studies. Paris: OECD; 2003. p. 19-85.
-
- Van Doorslaer E, Wagstaff A, Rutten F, editors. Equity in the finance and delivery of health care: an international perspective. Oxford: Oxford University Press; 1993.
-
- Eurostat. European Community Household Panel (ECHP): selected indicators from the 1995 wave. Luxembourg: European Commission, Eurostat; 1999.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources