

MR imaging and angiography of primary CNS vasculitis of childhood
- PMID: 16418382
- PMCID: PMC7976078
MR imaging and angiography of primary CNS vasculitis of childhood
Abstract
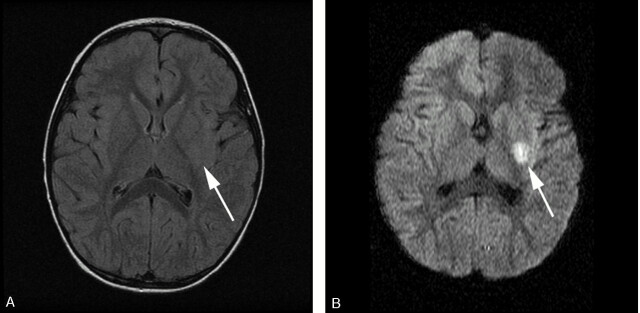
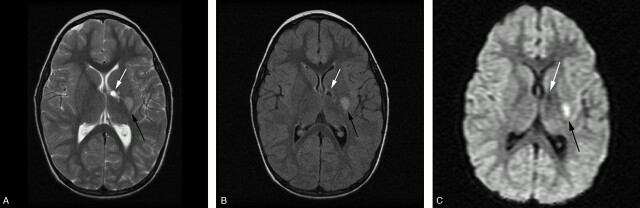
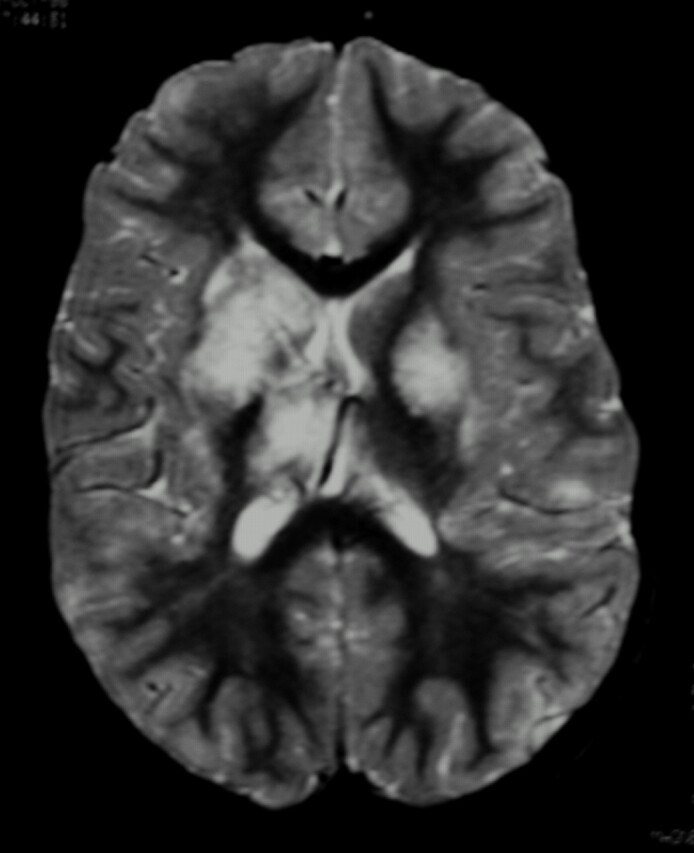
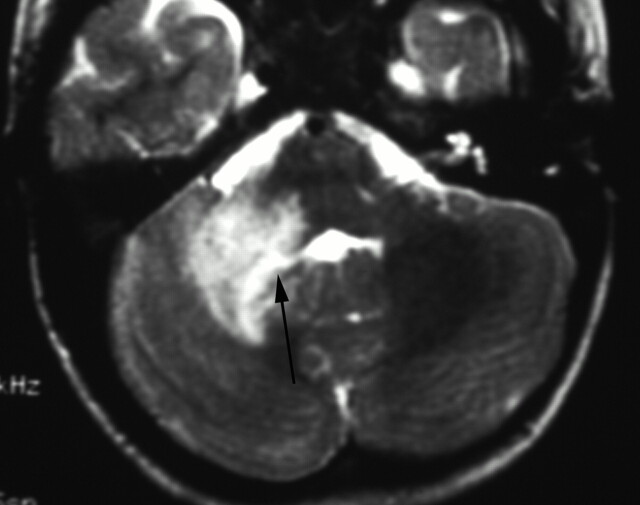
Background and purpose: Primary angiitis of the central nervous system of childhood (cPACNS) is a rare and ill-defined disease. In the absence of a brain biopsy, the diagnosis is based on typical clinical and imaging abnormalities. The aim of this study was to analyze systematically the MR imaging and MR angiographic (MRA) abnormalities in a large cohort of children with cPACNS.
Methods: We analyzed the MR imaging features of a single pediatric center cohort of 45 cPACNS patients. MR imaging studies were performed for all patients, and both MR imaging and MRA were performed for 42 patients, who formed the cohort for review of the presence and correlation of lesions. Proportions were calculated by using the Fisher exact test, and agreement between MR imaging and MRA was calculated by using the McNemar test. The sensitivity of each diagnostic technique was established.
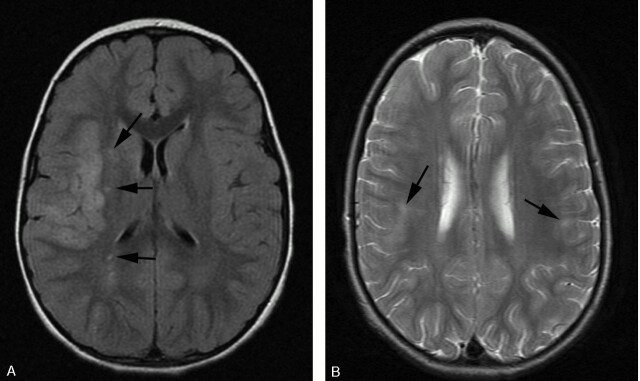
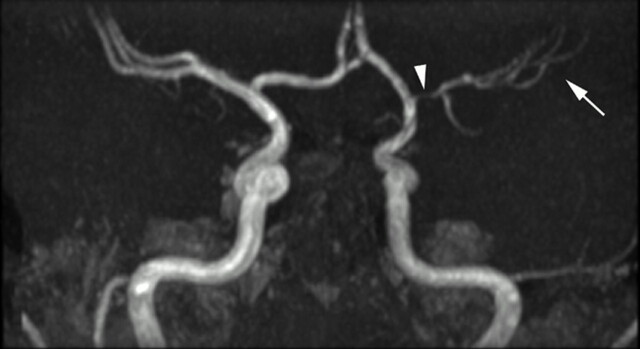
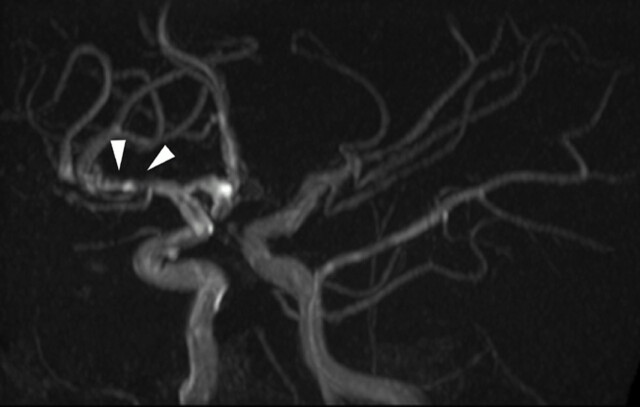
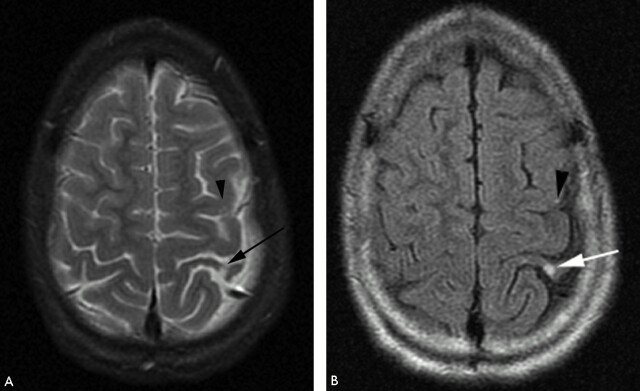
Results: The most-common pattern of parenchymal abnormality was multifocal, unilateral involvement, each in 42/45 patients (93%). The lateral lenticulostriate artery terrritory was affected in 56% of cases, with involvement of a supratentorial deep gray matter structure in 91%. No infratentorial lesion occurred in the absence of supratentorial abnormality. MRA was normal in 12/42 patients (28.6%). Among the abnormal studies, stenosis was detected on MRA in 83% and was "benign" in appearance in 73% of patients and "aggressive" in 16.7%. Involvement was proximal in 83% and distal in 27% of patients. Multiple ipsilateral lesions were seen in 63%. MR imaging was abnormal in every patient where MRA was abnormal. With the assumption of MR imaging as the gold standard, the sensitivity of MRA was 72%. The agreement between MR imaging and MRA for abnormality was significant (P = .04).
Conclusion: We have illustrated the MR imaging and MRA appearances of cPACNS in the largest cohort to date. Both parenchymal and vascular lesions were predominantly proximal, unilateral, and multifocal within the anterior circulation. There was good agreement between MR imaging and MRA for lesion location. MR imaging findings were abnormal in all cases at diagnosis, and this remains the most sensitive technique to the detection of vasculitis.
Figures
References
-
- Benseler S, Schneider R. Central nervous system vasculitis in children. Curr Opin Rheumatol 2004;16:43–50 - PubMed
-
- Pomper MG, Miller TJ, Stone JH, et al. CNS vasculitis in autoimmune disease: MR imaging findings and correlation with angiography. AJNR Am J Neuroradiol 1999;20:75–85 - PubMed
-
- Campi, Vollmer TL, Guarnaccia J, et al. Idiopathic granulomatous angiitis of the central nervous system: diagnostic challenges. Arch Neurol 1993;50:925–30 - PubMed
-
- Calabrese LH, Duna GF, Lie JT. Vasculitis in the central nervous system. Arthritis Rheum 1997;40:1189–1201 - PubMed
-
- Greenan TJ, Grossman RI, Goldberg HI. Cerebral vasculitis: MR imaging and angiographic correlation. Radiology 1992;182:65–72 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical