

Randomized controlled trial of an informatics-based intervention to increase statin prescription for secondary prevention of coronary disease
- PMID: 16423119
- PMCID: PMC1484624
- DOI: 10.1111/j.1525-1497.2005.00268.x
Randomized controlled trial of an informatics-based intervention to increase statin prescription for secondary prevention of coronary disease
Abstract
Objective: Suboptimal treatment of hyperlipidemia in patients with coronary artery disease (CAD) is well documented. We report the impact of a computer-assisted physician-directed intervention to improve secondary prevention of hyperlipidemia.
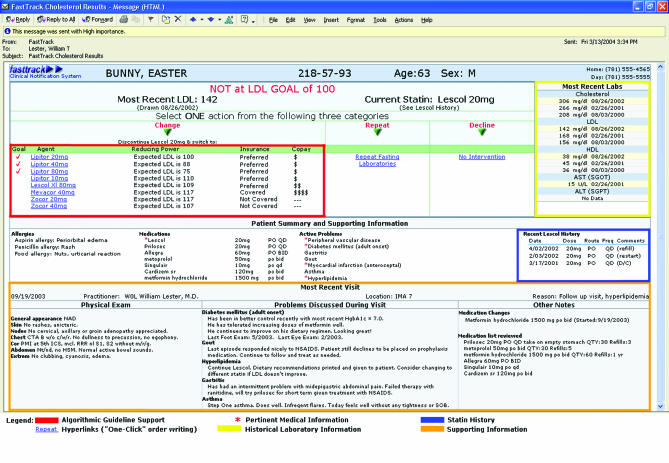
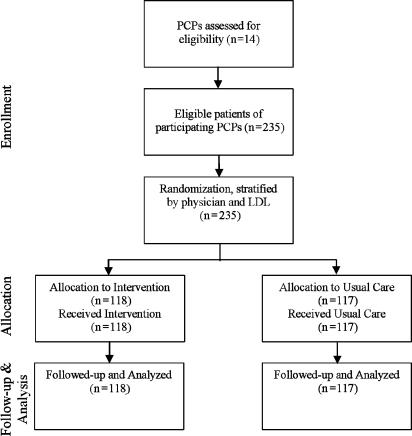
Design and setting: Two hundred thirty-five patients under the care of 14 primary care physicians in an academically affiliated practice with an electronic health record were enrolled in this proof-of-concept physician-blinded randomized, controlled trial. Each patient with CAD or risk equivalent above National Cholesterol Education Program-recommended low-density lipoprotein (LDL) treatment goal for greater than 6 months was randomized, stratified by physician and baseline LDL. Physicians received a single e-mail per intervention patient. E-mails were visit independent, provided decision support, and facilitated "one-click" order writing.
Measurements: The primary outcomes were changes in hyperlipidemia prescriptions, time to prescription change, and changes in LDL levels. The time spent using the system was assessed among intervention patients.
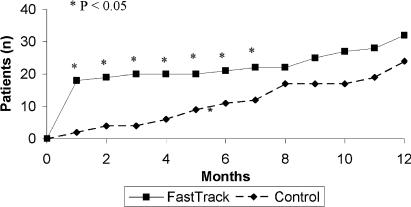
Results: A greater proportion of intervention patients had prescription changes at 1 month (15.3% vs 2%, P=.001) and 1 year (24.6% vs 17.1%, P=.14). The median interval to first medication adjustment occurred earlier among intervention patients (0 vs 7.1 months, P=.005). Among patients with baseline LDLs >130 mg/dL, the first postintervention LDLs were substantially lower in the intervention group (119.0 vs 138.0 mg/dL, P=.04). Physician processing time was under 60 seconds per e-mail.
Conclusion: A visit-independent disease management tool resulted in significant improvement in secondary prevention of hyperlipidemia at 1-month postintervention and showed a trend toward improvement at 1 year.
Figures
Comment in
-
A single email to clinicians may improve short-term prescribing for people with coronary artery disease and raised LDL cholesterol.Evid Based Cardiovasc Med. 2006 Jun;10(2):127-9. doi: 10.1016/j.ebcm.2006.04.031. Epub 2006 May 24. Evid Based Cardiovasc Med. 2006. PMID: 16753528 No abstract available.
References
-
- Committee on Quality of Health Care in America, Institute of Medicine. Crossing the Quality Chasm: A New Health System for the 21st Century Health Care Services. Washington, DC: National Academy Press; 2001.
-
- Braunwald E, et al. Shattuck lecture—cardiovascular medicine at the turn of the millennium:triumphs, concerns, and opportunities. N Engl J Med. 1997;337:1360–9. - PubMed
-
- McGlynn EA, Asch SM, Adams J, et al. The quality of health care delivered to adults in the United States. N Engl J Med. 2003;348:2635–45. - PubMed
-
- Grant RW, Cagliero E, Murphy-Sheehy P, Singer DE, Nathan DM, Meigs JB, et al. Comparison of hyperglycemia, hypertension, and hypercholesterolemia management in patients with type 2 diabetes. Am J Med. 2002;112:603–9. - PubMed
-
- Grant RW, Cagliero E, Dubey A, et al. Clinical inertia in the management of type 2 diabetes metabolic risk factors. Diabetic Med. 2004;21:150–5. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous