

Contrast-enhanced multidetector computed tomography viability imaging after myocardial infarction: characterization of myocyte death, microvascular obstruction, and chronic scar
- PMID: 16432071
- PMCID: PMC3410562
- DOI: 10.1161/CIRCULATIONAHA.105.521450
Contrast-enhanced multidetector computed tomography viability imaging after myocardial infarction: characterization of myocyte death, microvascular obstruction, and chronic scar
Abstract
Background: The ability to distinguish dysfunctional but viable myocardium from nonviable tissue has important prognostic implications after myocardial infarction. The purpose of this study was to validate the accuracy of contrast-enhanced multidetector computed tomography (MDCT) for quantifying myocardial necrosis, microvascular obstruction, and chronic scar after occlusion/reperfusion myocardial infarction.
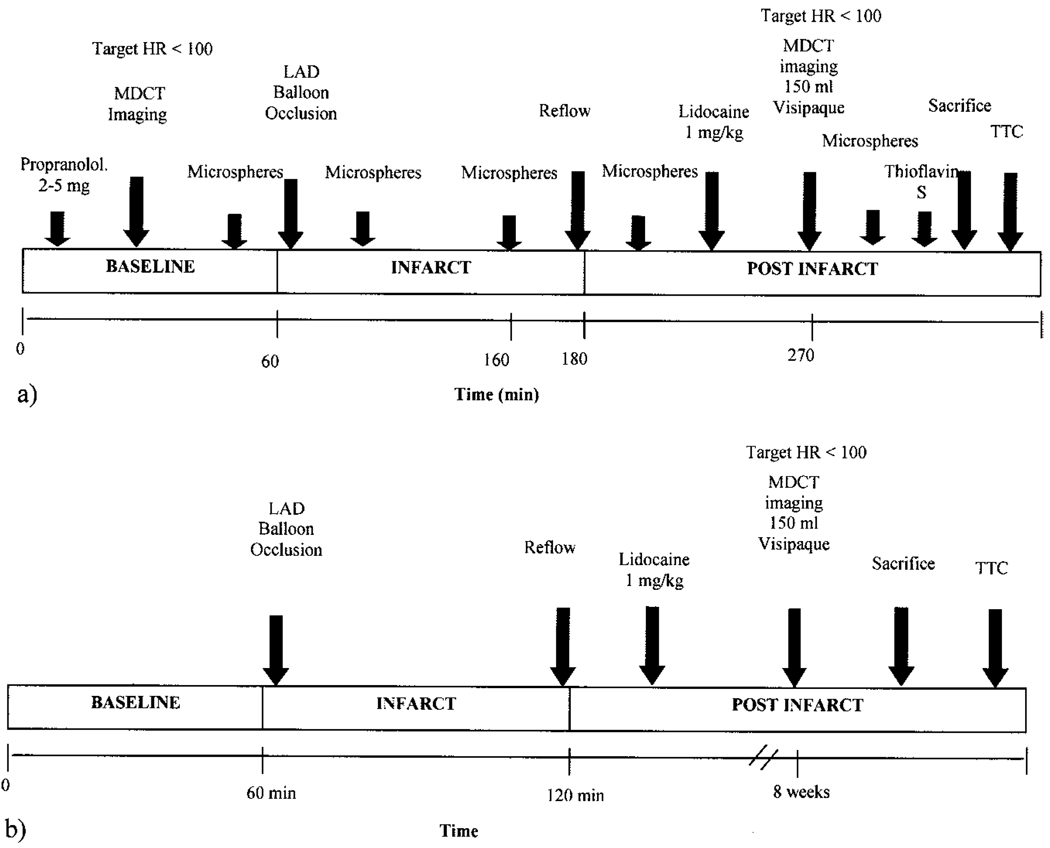
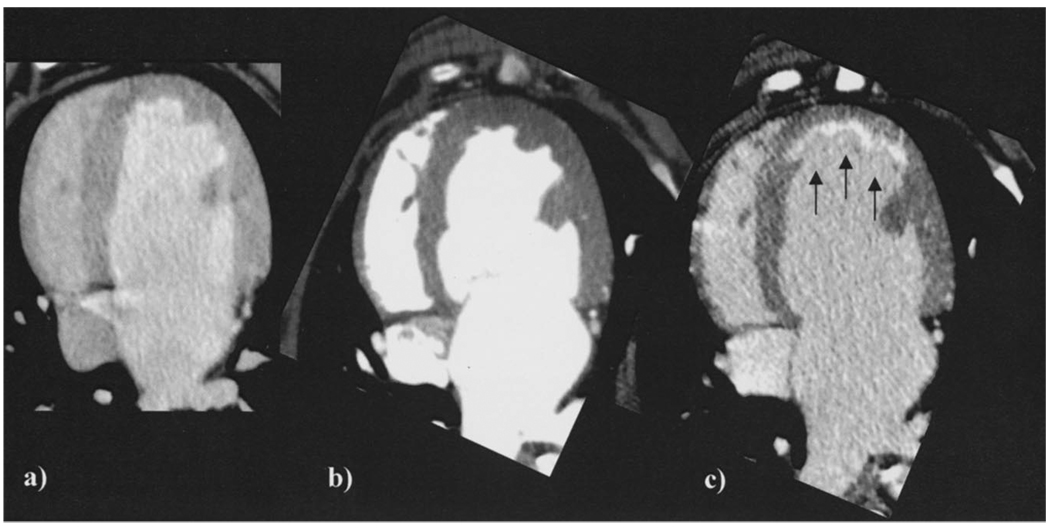
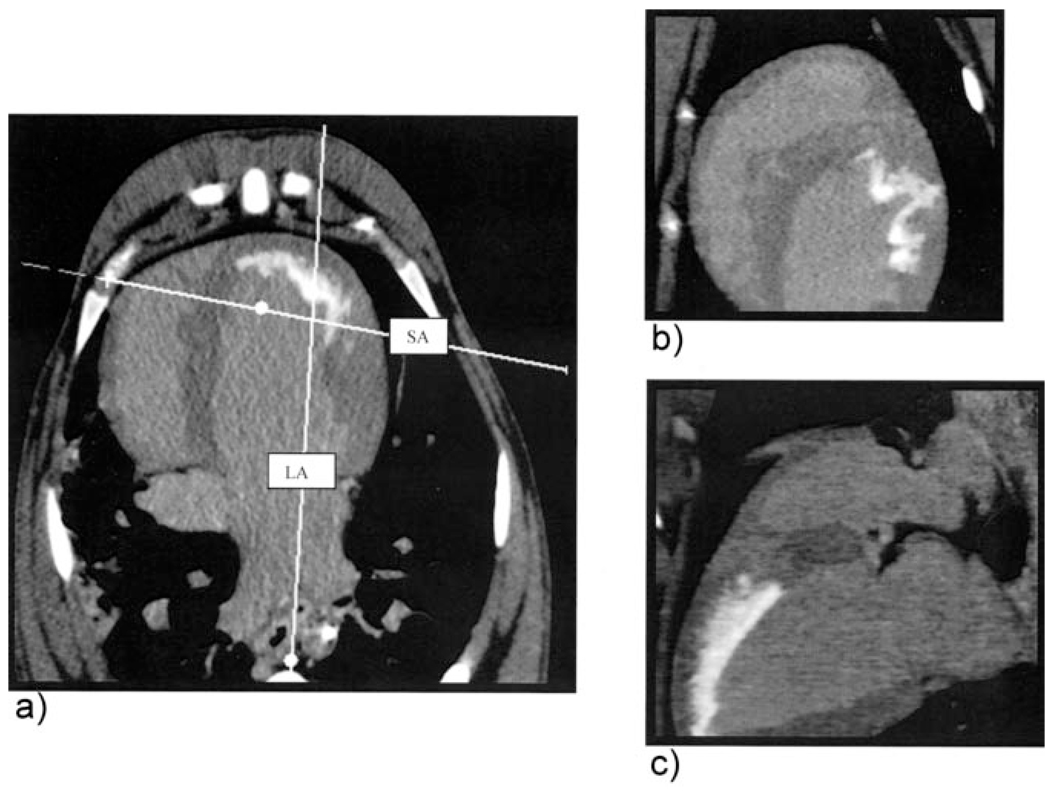
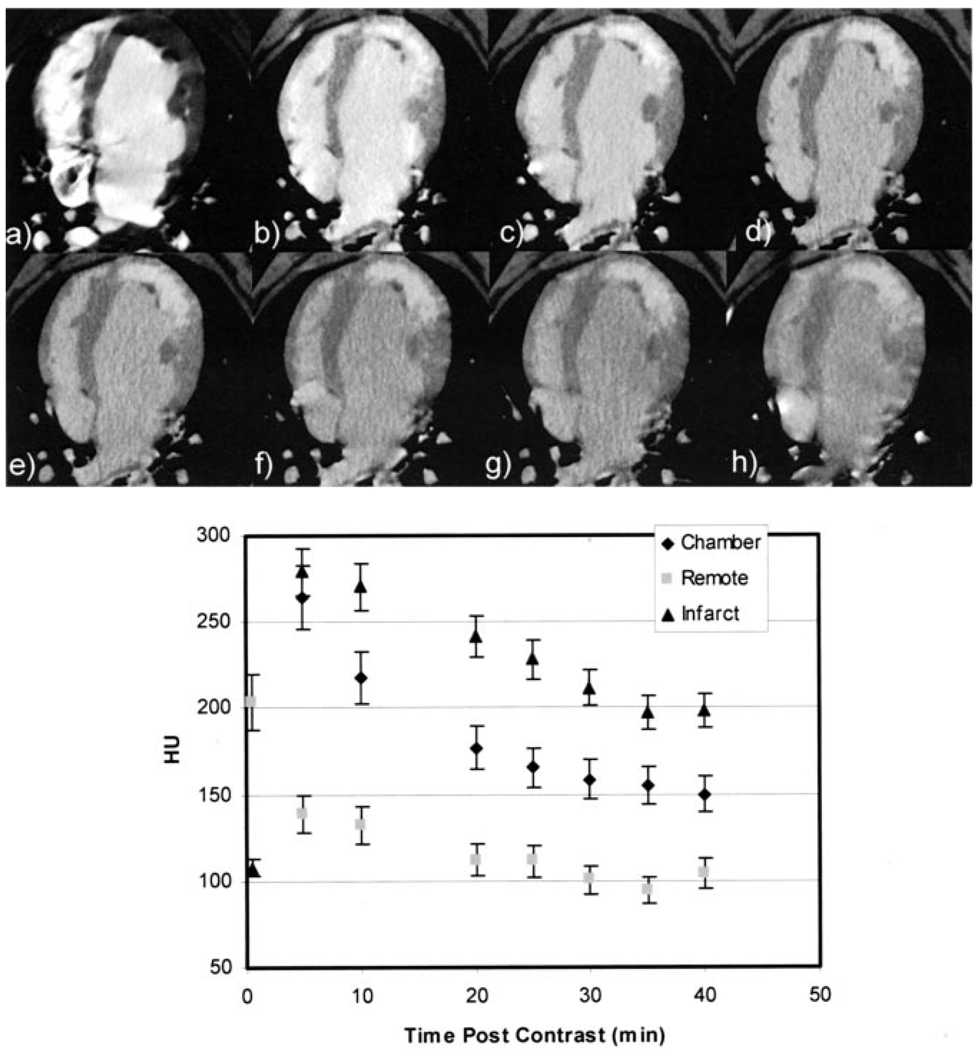
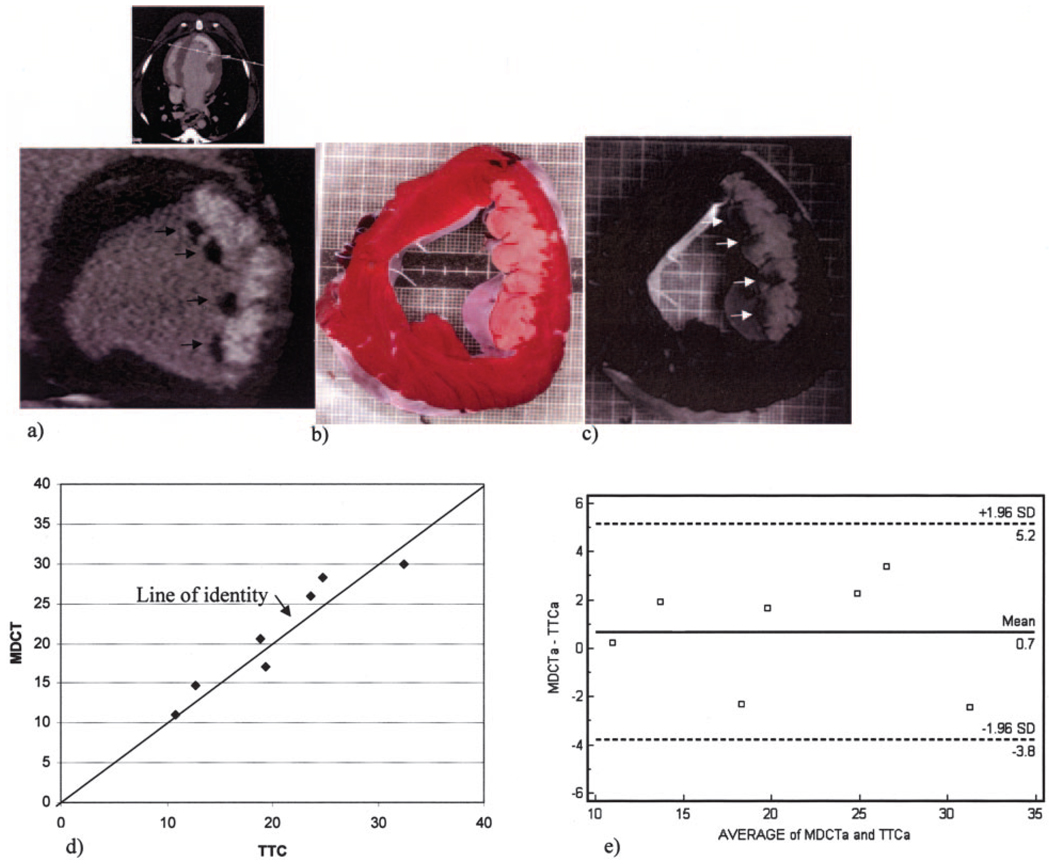
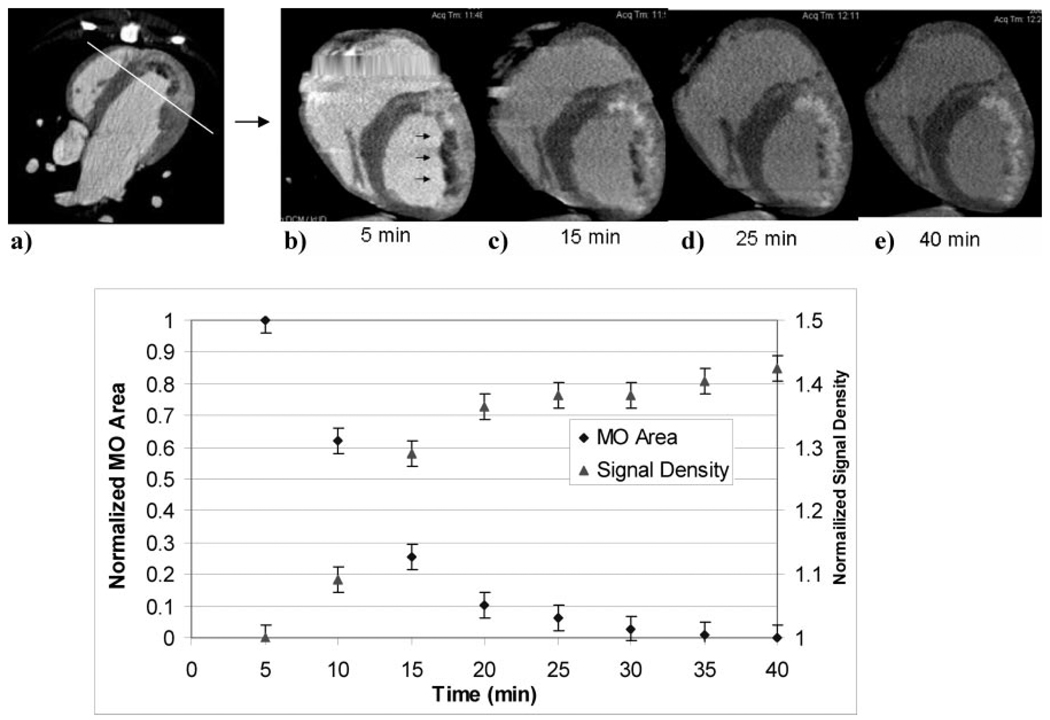
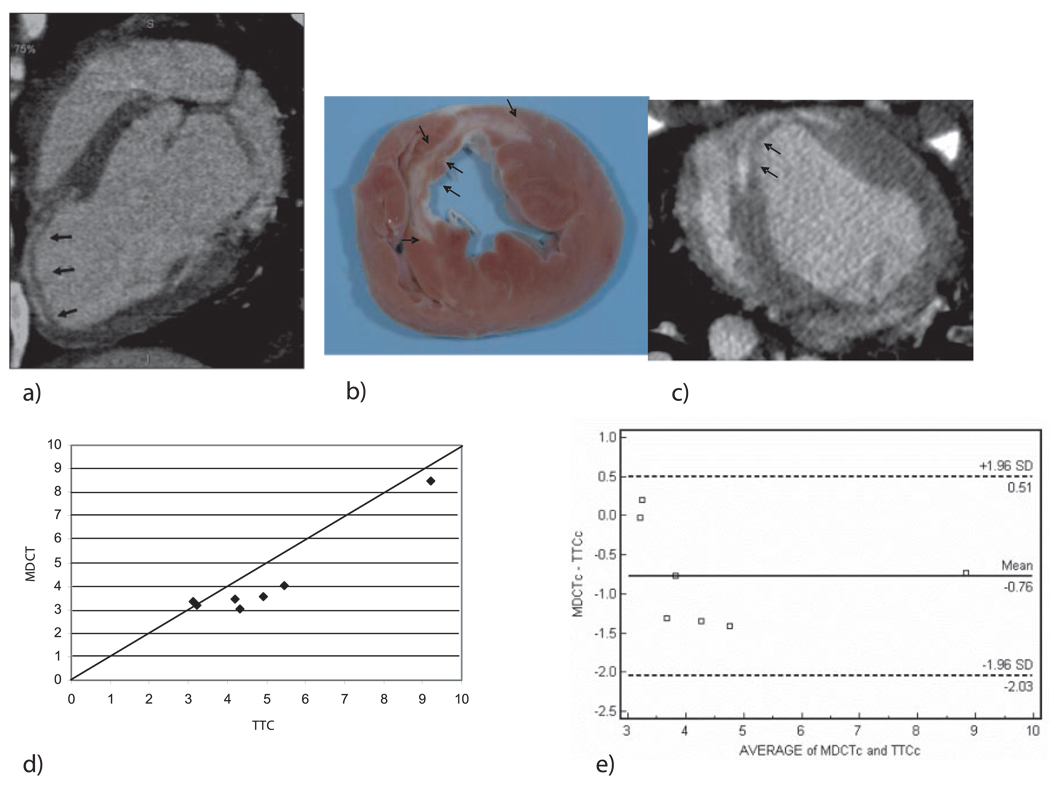
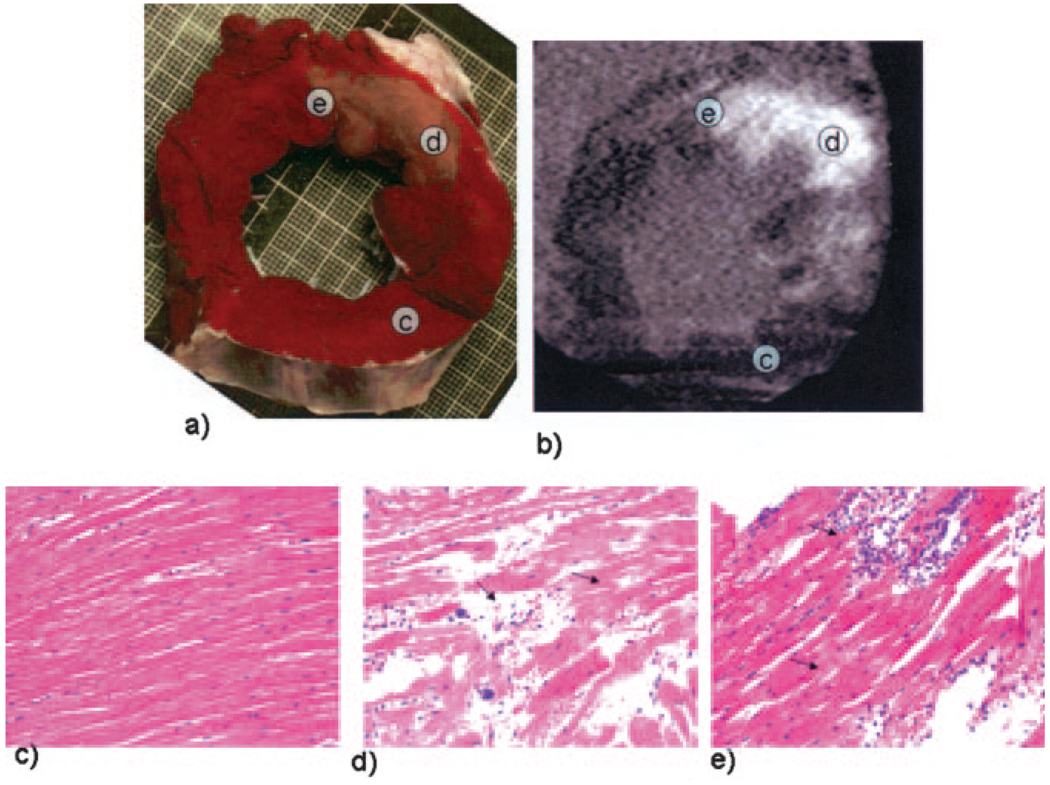
Methods and results: Ten dogs and 7 pigs underwent balloon occlusion of the left anterior descending coronary artery (LAD) followed by reperfusion. Contrast-enhanced (Visipaque, 150 mL, 325 mg/mL) MDCT (0.5 mm x 32 slice) was performed before occlusion and 90 minutes (canine) or 8 weeks (porcine) after reperfusion. MDCT images were analyzed to define infarct size/extent and microvascular obstruction and compared with postmortem myocardial staining (triphenyltetrazolium chloride) and microsphere blood flow measurements. Acute and chronic infarcts by MDCT were characterized by hyperenhancement, whereas regions of microvascular obstruction were characterized by hypoenhancement. MDCT infarct volume compared well with triphenyltetrazolium chloride staining (acute infarcts 21.1+/-7.2% versus 20.4+/-7.4%, mean difference 0.7%; chronic infarcts 4.15+/-1.93% versus 4.92+/-2.06%, mean difference -0.76%) and accurately reflected morphology and the transmural extent of injury in all animals. Peak hyperenhancement of infarcted regions occurred approximately 5 minutes after contrast injection. MDCT-derived regions of microvascular obstruction were also identified accurately in acute studies and correlated with reduced flow regions as measured by microsphere blood flow.
Conclusions: The spatial extent of acute and healed myocardial infarction can be determined and quantified accurately with contrast-enhanced MDCT. This feature, combined with existing high-resolution MDCT coronary angiography, may have important implications for the comprehensive assessment of cardiovascular disease.
Conflict of interest statement
Drs Lardo and Lima receive research support from Toshiba, Inc. The other authors report no conflicts.
Figures
References
-
- Alderman EL, Fisher LD, Litwin P, Kaiser GC, Myers WO, Maynard C, Levine F, Schloss M. Results of coronary artery surgery in patients with poor left ventricular function (CASS) Circulation. 1983;68:785–795. - PubMed
-
- Pagley PR, Beller GA, Watson DD, Gimple LW, Ragosta M. Improved outcome after coronary bypass surgery in patients with ischemic cardiomyopathy and residual myocardial viability. Circulation. 1997;96:793–800. - PubMed
-
- Bax JJ, Schinkel AF, Boersma E, Rizzello V, Elhendy A, Maat A, Roelandt JR, van der Wall EE, Poldermans D. Early versus delayed revascularization in patients with ischemic cardiomyopathy and sub-stantial viability: impact on outcome. Circulation. 2003;108(suppl I):II-39–II-42. - PubMed
-
- Kim RJ, Wu E, Rafael A, Chen EL, Parker MA, Simonetti O, Klocke FJ, Bonow RO, Judd RM. The use of contrast-enhanced magnetic resonance imaging to identify reversible myocardial dysfunction. N Engl J Med. 2000;343:1445–1453. - PubMed
-
- Wu KC, Lima JA. Noninvasive imaging of myocardial viability: current techniques and future developments. Circ Res. 2003;93:1146–1158. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
