

The immune paradox of sarcoidosis and regulatory T cells
- PMID: 16432251
- PMCID: PMC2118208
- DOI: 10.1084/jem.20050648
The immune paradox of sarcoidosis and regulatory T cells
Erratum in
- J Exp Med. 2006 Feb 20;203(2):477
Abstract
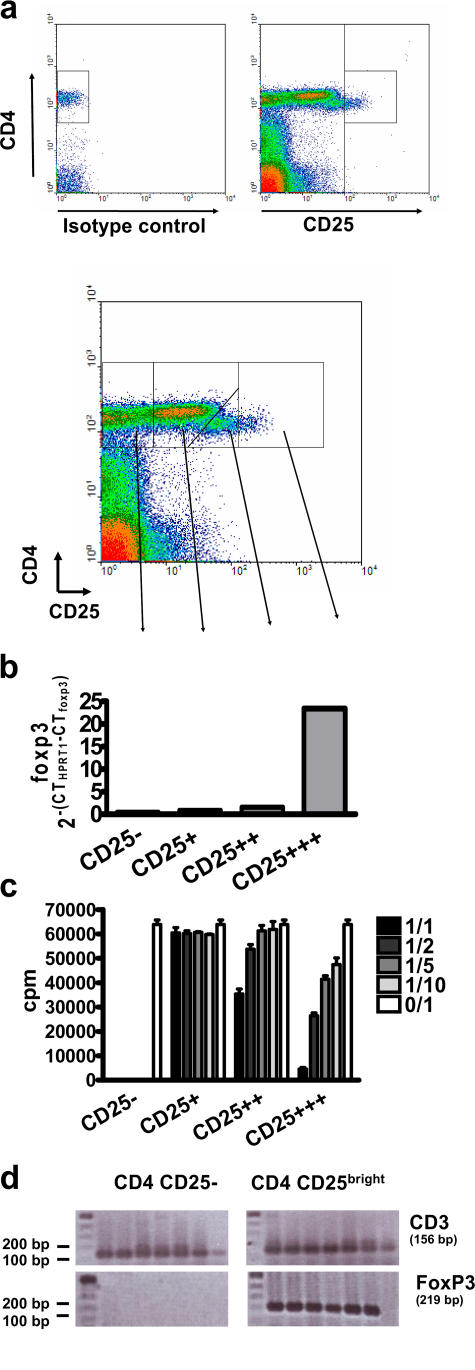
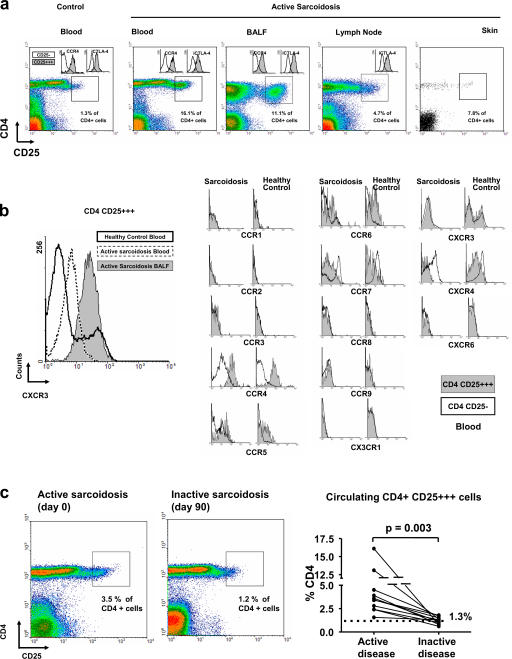
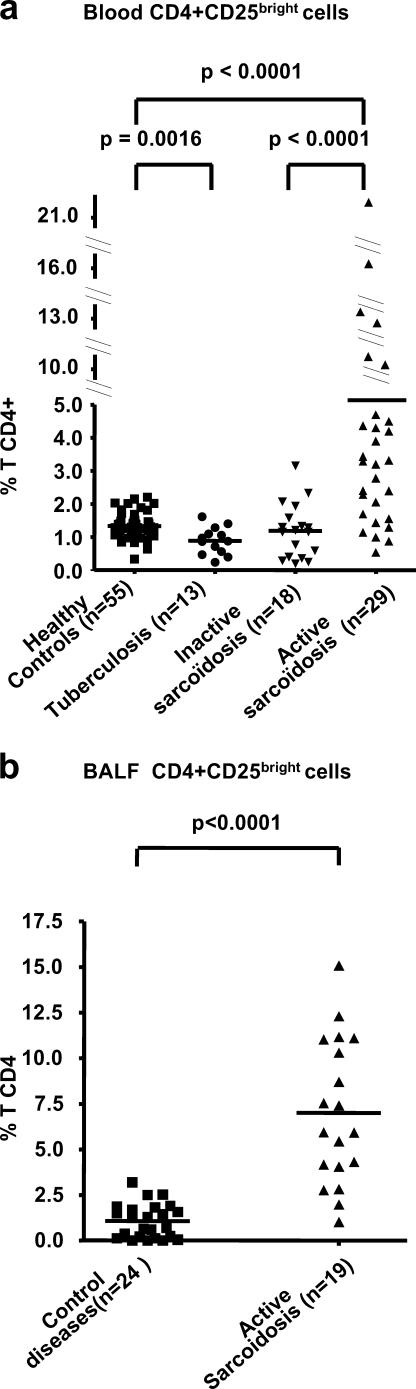
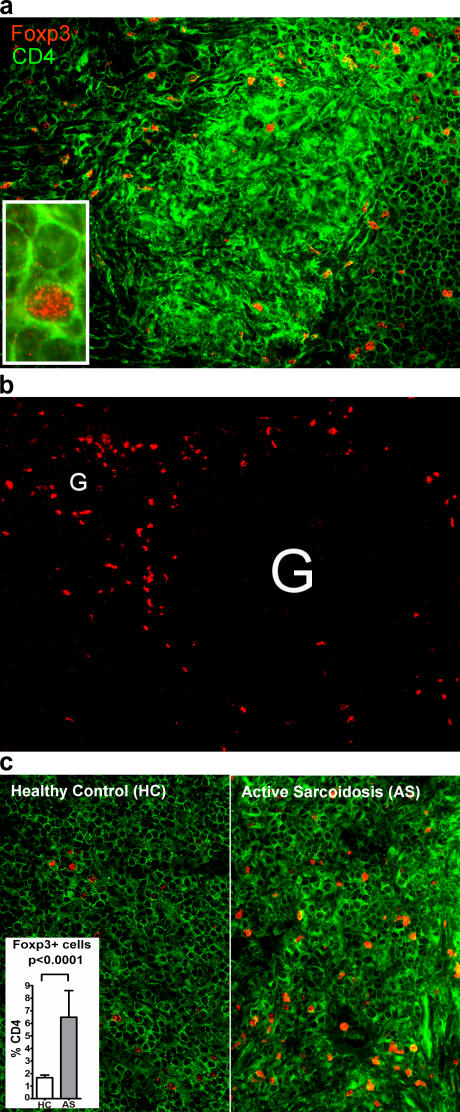
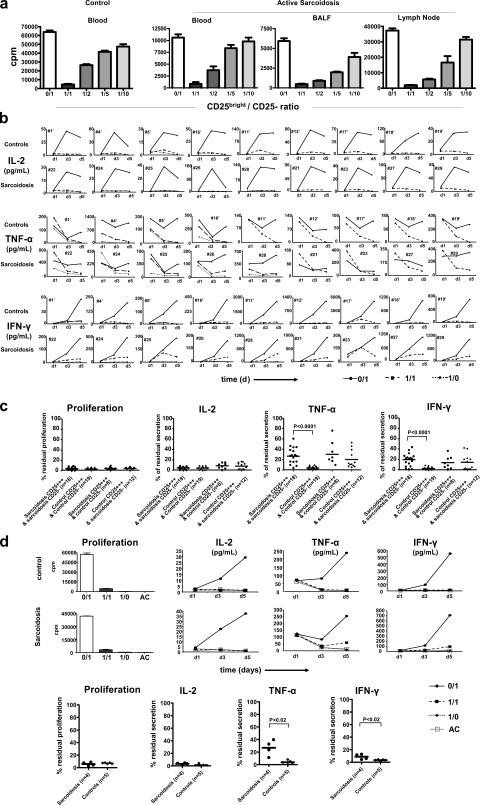
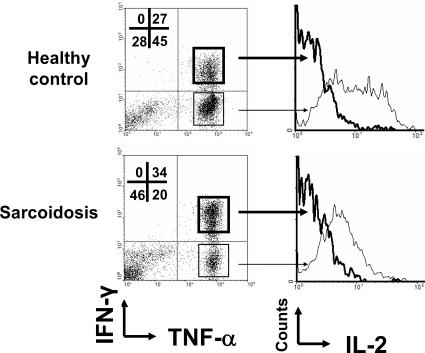
Sarcoidosis is characterized by extensive local inflammation (granuloma, cytokine secretion) associated with anergy (poor response to antigens in vitro and in vivo). We postulated that this paradoxical situation would correspond to a disequilibrium between effector and regulatory T lymphocytes (T reg cells). We show that CD4+CD25(bright)FoxP3+ cells accumulate at the periphery of sarcoid granulomas, in bronchoalveolar lavage fluid, and in peripheral blood of patients with active disease. These cells exhibited powerful antiproliferative activity, yet did not completely inhibit TNF-alpha production. Sarcoidosis is therefore associated with a global T reg cell subset amplification whose activity would be insufficient to control local inflammation. At the same time, peripheral T reg cells exert powerful antiproliferative activity that may account for the state of anergy. Altogether, these findings advance our conceptual understanding of immune regulation in a way that resolves the immune paradox of sarcoidosis and permit us to envisage a profound clinical impact of T reg cell manipulation on immunity.
Figures
References
-
- Hunninghake, G.W., and R.G. Crystal. 1981. Pulmonary sarcoidosis: a disorder mediated by excess helper T-lymphocyte activity at sites of disease activity. N. Engl. J. Med. 305:429–434. - PubMed
-
- Baumer, I., G. Zissel, M. Schlaak, and J. Muller-Quernheim. 1997. Th1/Th2 cell distribution in pulmonary sarcoidosis. Am. J. Respir. Cell Mol. Biol. 16:171–177. - PubMed
-
- Newman, L.S., C.S. Rose, and L.A. Maier. 1997. Sarcoidosis. N. Engl. J. Med. 336:1224–1234. - PubMed
-
- Baughman, R.P., E.E. Lower, and R.M. du Bois. 2003. Sarcoidosis. Lancet. 361:1111–1118. - PubMed
-
- Lecossier, D., D. Valeyre, A. Loiseau, J. Cadranel, A. Tazi, J.P. Battesti, and A.J. Hance. 1991. Antigen-induced proliferative response of lavage and blood T lymphocytes. Comparison of cells from normal subjects and patients with sarcoidosis. Am. Rev. Respir. Dis. 144:861–868. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
