

Evidence-based treatment of acute pancreatitis: a look at established paradigms
- PMID: 16432347
- PMCID: PMC1448904
- DOI: 10.1097/01.sla.0000197334.58374.70
Evidence-based treatment of acute pancreatitis: a look at established paradigms
Abstract
Background: The management of acute pancreatitis (AP) is still based on speculative and unproven paradigms in many centers. Therefore, we performed an evidence-based analysis to assess the best available treatment.
Methods: A comprehensive Medline and Cochrane Library search was performed evaluating the indication and timing of interventional and surgical approaches, and the value of aprotinin, lexipafant, gabexate mesylate, and octreotide treatment. Each study was ranked according to the evidence-based methodology of Sackett; whenever feasible, we performed new meta-analyses using the random-effects model. Recommendations were based on the available level of evidence (A=large randomized; B=small randomized; C=prospective trial).
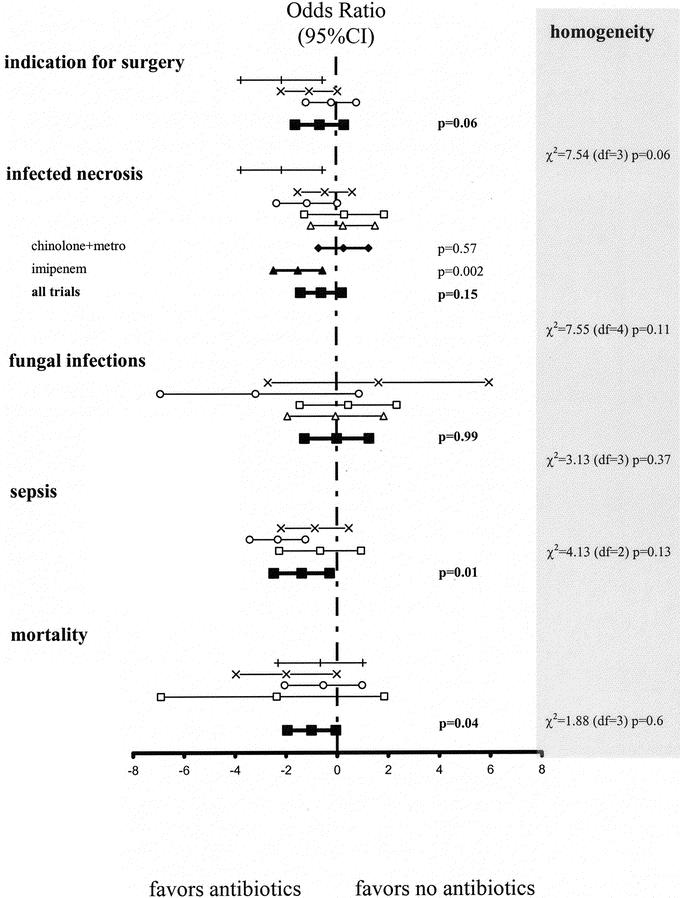
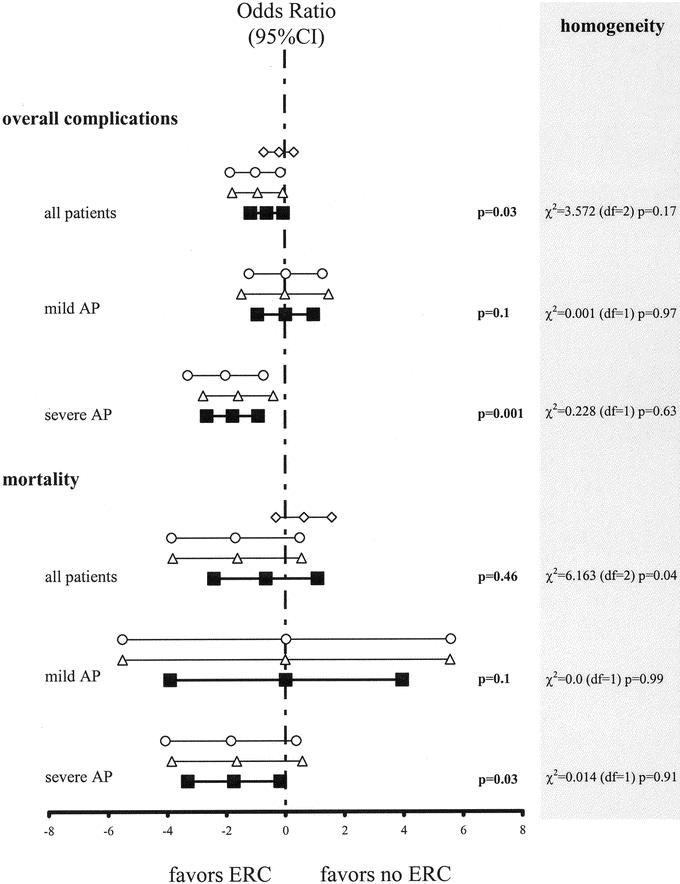
Results: None of the evaluated medical treatments is recommended (level A). Patients with AP should receive early enteral nutrition (level B). While mild biliary AP is best treated by primary cholecystectomy (level B), patients with severe biliary AP require emergency endoscopic papillotomy followed by interval cholecystectomy (level A). Patients with necrotizing AP should receive imipenem or meropenem prophylaxis to decrease the risk of infected necrosis and mortality (level A). Sterile necrosis per se is not an indication for surgery (level C), and not all patients with infected necrosis require immediate surgery (level B). In general, early necrosectomy should be avoided (level B), and single necrosectomy with postoperative lavage should be preferred over "open-packing" because of fewer complications with comparable mortality rates (level C).
Conclusions: While providing new insights into key aspects of AP management, this evidence-based analysis highlights the need for further clinical trials, particularly regarding the indications for antibiotic prophylaxis and surgery.
Figures
Comment in
-
Evidence-based treatment of acute pancreatitis: antibiotic prophylaxis in necrotizing pancreatitis.Ann Surg. 2006 Oct;244(4):637-8; author reply 638-9. doi: 10.1097/01.sla.0000239627.78772.f7. Ann Surg. 2006. PMID: 16998381 Free PMC article. No abstract available.
References
-
- Steinberg W, Tenner S. Acute pancreatitis. N Engl J Med. 1994;330:1198–1210. - PubMed
-
- Lankisch PG. Epidemiology of acute pancreatitis. In: Malfertheimer P, ed. Acute Pancreatitis: Novel Concepts in Biology and Therapy, 1st ed. Berlin: Blackwell Science, 1999:145–153.
-
- Bank S, Singh P, Pooran N, et al. Evaluation of factors that have reduced mortality from acute pancreatitis over the past 20 years. J Clin Gastroenterol. 2002;35:50–60. - PubMed
-
- Soran A, Chelluri L, Lee KKW, et al. Outcome and quality of life of patients with acute pancreatitis requiring intensive care. J Surg Res. 2000;91:89–94. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
