

Potential value of contrast-enhanced intraoperative ultrasonography during partial hepatectomy for metastases: an essential investigation before resection?
- PMID: 16432357
- PMCID: PMC1448920
- DOI: 10.1097/01.sla.0000197708.77063.07
Potential value of contrast-enhanced intraoperative ultrasonography during partial hepatectomy for metastases: an essential investigation before resection?
Abstract
Objective: The aim of the study was to assess the clinical value of contrast-enhanced intraoperative ultrasound (CE-IOUS) as a novel tool in the hepatic staging of patients undergoing liver resection.
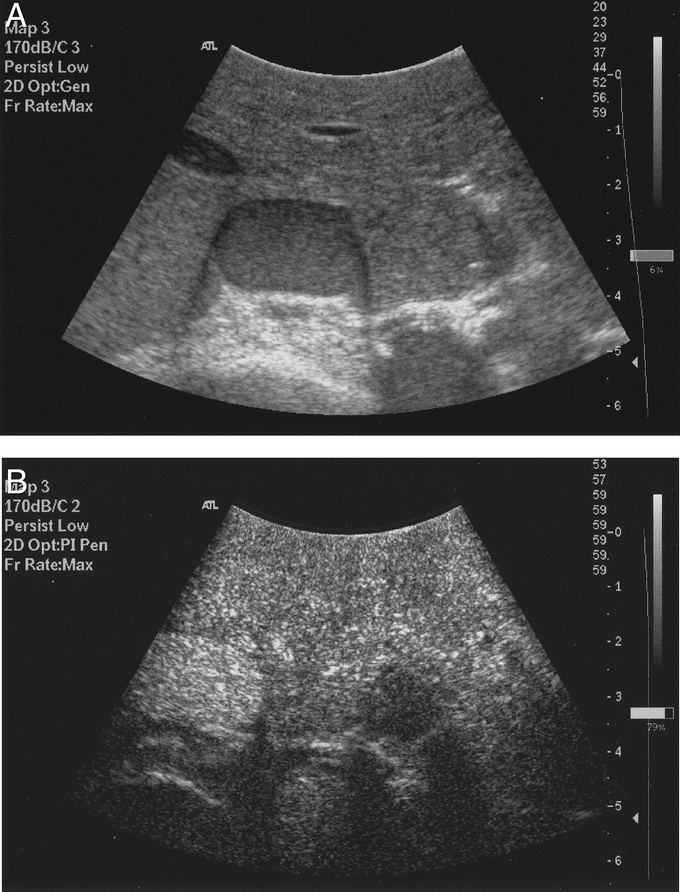
Methods: Sixty patients scheduled to undergo liver resection for metastatic disease were studied. Preoperative staging with contrast-enhanced CT and/or MR scans was performed within 2 to 6 weeks of operation. Following exploration, intraoperative ultrasound (IOUS) was performed using an HDI-5000 scanner (Philips) and a finger-probe with pulse inversion harmonic (PIH) capability. CE-IOUS in the PIH mode was performed in a standardized protocol (low MI: 0.02-0.04) after intravenous injection of 3-4 mL of SonoVue (Bracco spa, Milan); all detected lesions on precontrast and postcontrast scans were counted and mapped. Any alteration in surgical management was documented following CE-IOUS compared with IOUS.
Results: Three patients were excluded due to disseminated disease on exploration. CE-IOUS was significantly more sensitive than CT/MR and IOUS in detecting liver metastases (96.1% versus 76.7% and 81.5%, respectively) (P<0.05); it altered surgical management in 29.8% (17 of 57) of cases, due to 1) additional metastases in 19.3% (11 of 57), 2) less metastases in 3.5% (2 of 57), 3) benign lesions wrongly diagnosed as metastasis on IOUS/CT in 5.3% (3 of 57), and 4) vascular proximity in 1.8% (1 of 57). Management was unchanged in 70.2% (40 of 57) despite additional lesions detected in 3.5% (2 of 57) and benign lesion wrongly diagnosed on IOUS and CT as metastasis in 1.8% (1 of 57). CE-IOUS altered combined IOUS/CT/MR staging in 35.1%.
Conclusion: These preliminary results suggest CE-IOUS is an essential tool prior to liver resection for metastases.
Comment in
-
Contrast-enhanced intraoperative ultrasonography: a valuable and not any more monocentric diagnostic technique performed in different ways.Ann Surg. 2007 Jan;245(1):152-3; author reply 152-3. doi: 10.1097/01.sla.0000250940.21627.57. Ann Surg. 2007. PMID: 17197980 Free PMC article. No abstract available.
References
-
- O'Brien MJ. Cancer of the colon and rectum: current concepts of etiology and pathogenesis. Br J Med Sci. 1988;157:5–15. - PubMed
-
- McArdle CS, Hole D, Hansell D, et al. A prospective study of colorectal cancer in the West of Scotland: a ten year follow-up. Br J Surg. 1990;77:206–208. - PubMed
-
- Scheele J, Strang R, Altendorf-Hofmann A, et al. Resection of colorectal liver metastases. World J. Surg. 1995;19:59–71. - PubMed
-
- Fong Y, Cohen AM, Fortner JG, et al. Liver resection for colorectal metastases. J Clin Oncol. 1997;15:938–46. - PubMed
-
- Finlay IG, Meek D, Brunton F, et al. Growth rate of hepatic metastases in colorectal carcinoma. Br J Surg. 1988;75:641–644. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
