

Race and surgical mortality in the United States
- PMID: 16432363
- PMCID: PMC1448914
- DOI: 10.1097/01.sla.0000197560.92456.32
Race and surgical mortality in the United States
Abstract
Objective: This study describes racial differences in postoperative mortality following 8 cardiovascular and cancer procedures and assesses possible explanations for these differences.
Summary background data: Although racial disparities in the use of surgical procedures are well established, relationships between race and operative mortality have not been assessed systematically.
Methods: We used national Medicare data to identify all patients undergoing one of 8 cardiovascular and cancer procedures between 1994 and 1999. We used multiple logistic regression to assess differences in operative mortality (death within 30 days or before discharge) between black patients and white patients, controlling for patient characteristics. Adding hospital indicators to these models, we then assessed the extent to which racial differences in operative mortality could be accounted for by the hospital in which patients were cared for.
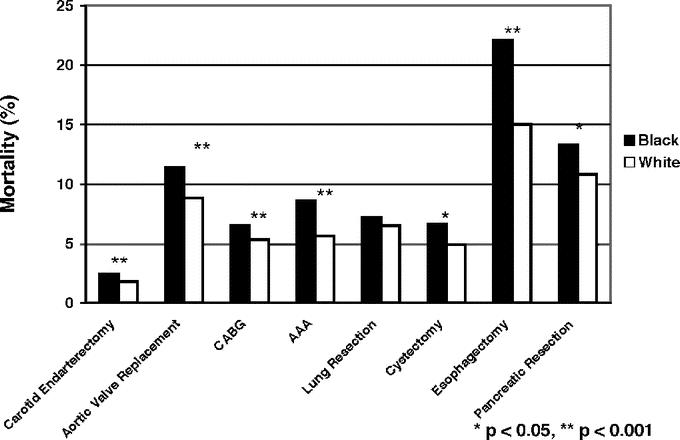
Results: Black patients had higher crude mortality rates than white patients for 7 of the 8 operations, including coronary artery bypass, aortic valve replacement, abdominal aortic aneurysm repair, carotid endarterectomy, radical cystectomy, pancreatic resection, and esophagectomy. Among these 7 procedures, odds ratios of mortality (black versus white) ranged from 1.23 (95% confidence interval, 1.18-1.29) for CABG to 1.61 (95% confidence interval, 1.28-2.03) for esophagectomy. Adjusting for patient characteristics had modest or no effect on odds ratios of mortality by race. However, there remained few clinically or statistically significant differences in mortality by race after we accounted for hospital. Hospitals that treated a large proportion of black patients had higher mortality rates for all 8 procedures, for white as well as black patients.
Conclusions: Black patients have higher operative mortality risks across a wide range of surgical procedures, in large part because of higher mortality rates at the hospitals they attend.
Figures
References
-
- Agency for Healthcare Research and Quality. National Healthcare Disparities Report. Rockville, MD: Agency for Healthcare Research and Quality, 2003.
-
- Smedley B, Stith A, Nelson A. Unequal Treatment: Confronting Racial and Ethnic Disparities in Health Care. Washington, DC: National Academies Press, 2003. - PubMed
-
- Gornick ME, Eggers PW, Reilly TW, et al. Effects of race and income on mortality and use of services among Medicare beneficiaries. N Engl J Med. 1996;335:791–799. - PubMed
-
- Peterson ED, Shaw LK, DeLong ER, et al. Racial variation in the use of coronary-revascularization procedures. Are the differences real? Do they matter? N Engl J Med. 1997;336:480–486. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
