

Interpatient variability in the pharmacokinetics of the HIV non-nucleoside reverse transcriptase inhibitor efavirenz: the effect of gender, race, and CYP2B6 polymorphism
- PMID: 16433869
- PMCID: PMC1885008
- DOI: 10.1111/j.1365-2125.2005.02536.x
Interpatient variability in the pharmacokinetics of the HIV non-nucleoside reverse transcriptase inhibitor efavirenz: the effect of gender, race, and CYP2B6 polymorphism
Abstract
Aims: To characterize the demographic and pharmacogenetic factors that influence interpatient variability in the plasma concentrations of the HIV non-nucleoside reverse transcriptase inhibitor efavirenz.
Methods: Data from all samples analyzed for efavirenz in our TDM service in 2002 and 2003 were reviewed. Information on gender, age, body weight, height, race, hormonal contraceptive use (in a subset of patients), and time between sampling and last intake was recorded. PCR-restriction fragment length polymorphism analysis was performed to detect the cytochrome P450 2B6 (CYP2B6) C1459T variant (present in CYP2B6*6 and CYP2B6*7) which is associated with low CYP2B6 activity.
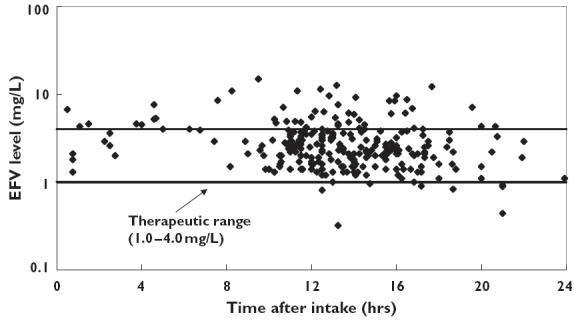
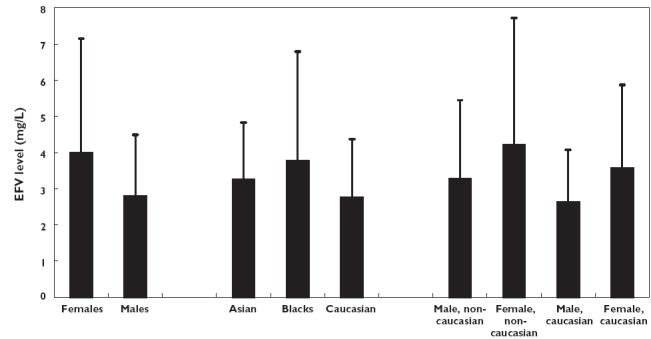
Results: A total of 255 patients were included in this analysis. The median plasma efavirenz concentration was 2.50 (interquartile range: 1.85-3.55) mg l(-1). Eight patients (3.1%) were considered to have a subtherapeutic plasma concentration (<1.0 mg l(-1)) and 48 (18.9%) a toxic efavirenz concentration (>4.0 mg l(-1)). Gender, time after last intake, and race were the only factors that were significantly related to plasma efavirenz concentration in a multivariate analysis. No influence was observed for body weight, hormonal contraceptive use, and the presence of the CYP2B6 C1459T polymorphism.
Conclusions: Gender and race are important factors in determining interpatient variability in plasma efavirenz concentrations which were unaffected by the presence of the CYP2B6 C1459T polymorphism. Physicians should be particularly alert for signs of efavirenz-induced toxicity in females and non-Caucasian patients.
Figures
References
-
- Panel on clinical practices for treatment of HIV infection, convened by the Department of Health and Human Services DHHS. Guidelines for the Use of Antiretroviral Agents in HIV-1 Infected Adults and Adolescents. 2004. March 23.
-
- Staszewski S, Morales-Ramirez J, Tashima KT, Rachlis A, Skiest D, Stanford J, Stryker R, Johnson P, Labriola DF, Farina D, Manion DJ, Ruiz NM. Efavirenz plus zidovudine and lamivudine, efavirenz plus indinavir, and indinavir plus zidovudine and lamivudine in the treatment of HIV-1 infection in adults. Study 006 Team. N Engl J Med. 1999;341:1865–73. - PubMed
-
- Van Leth F, Phanuphak P, Ruxrungtham K, Baraldi E, Miller S, Gazzard B, Cahn P, Lalloo UG, van der Westhuizen IP, Malan DR, Johnson MA, Santos BR, Mulcahy F, Wood R, Levi GC, Reboredo G, Squires K, Cassetti I, Petit D, Raffi F, Katlama C, Murphy RL, Horban A, Dam JP, Hassink E, van Leeuwen R, Robinson P, Wit FW, Lange JM. Comparison of first-line antiretroviral therapy with regimens including nevirapine, efavirenz, or both drugs, plus stavudine and lamivudine: a randomised open-label trial, the 2NN Study. Lancet. 2004;363:1253–63. - PubMed
-
- Gulick RM, Ribaudo HJ, Shikuma CM, Lustgarten S, Squires KE, Meyer WA, III, Acosta EP, Schackman BR, Pilcher CD, Murphy RL, Maher WE, Witt MD, Reichman RC, Snyder S, Klingman KL, Kuritzkes DR. Triple-nucleoside regimens versus efavirenz-containing regimens for the initial treatment of HIV-1 infection. N Engl J Med. 2004;350:1850–61. - PubMed
-
- Smith PF, DiCenzo R, Morse GD. Clinical pharmacokinetics of non-nucleoside reverse transcriptase inhibitors. Clin Pharmacokinet. 2001;40:893–905. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
