

Low levels of pyrazinamide and ethambutol in children with tuberculosis and impact of age, nutritional status, and human immunodeficiency virus infection
- PMID: 16436690
- PMCID: PMC1366879
- DOI: 10.1128/AAC.50.2.407-413.2006
Low levels of pyrazinamide and ethambutol in children with tuberculosis and impact of age, nutritional status, and human immunodeficiency virus infection
Abstract
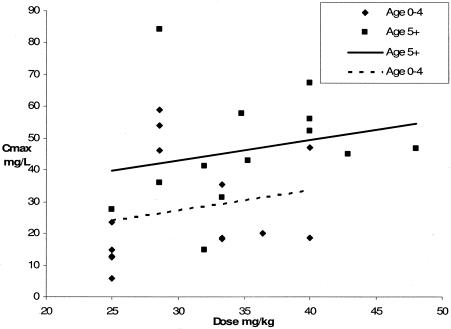
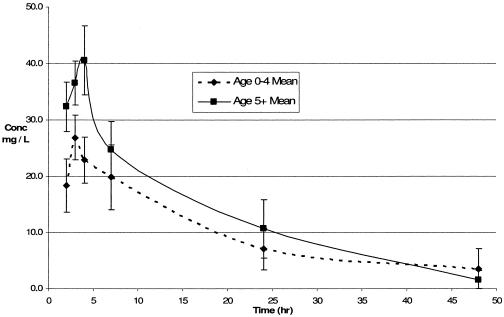
Recent pharmacokinetic studies that included children found that serum drug levels were low compared to those of adults for whom the same dosages were used. This study aimed to characterize the pharmacokinetics of pyrazinamide and ethambutol in Malawian children and to examine the impact of age, nutritional status, and human immunodeficiency virus (HIV) infection. We conducted a pharmacokinetic study of children treated for tuberculosis with thrice-weekly pyrazinamide (n = 27; mean age, 5.7 years) and of a separate group of children treated with thrice-weekly ethambutol (n = 18; mean age, 5.5 years) as portions of tablets according to national guidelines. Malnutrition and HIV infection were common in both groups. Blood samples were taken just prior to oral administration of the first dose, and subsequent samples were taken at intervals of 2, 3, 4, 7, 24, and 48 h after drug administration. Serum drug levels were low in all children for both drugs; in almost all cases, the maximum concentration of the drug in serum (Cmax) failed to reach the MIC for Mycobacterium tuberculosis. The Cmax of pyrazinamide was significantly lower in younger children (<5 years) than in older children. The Cmax of pyrazinamide was also lower for HIV-infected children and children with severe malnutrition, but these differences did not reach statistical significance. No differences were found for ethambutol in relation to age, HIV infection, or malnutrition, but the Cmax was <2 mg/liter in all cases. Studies of pharmacokinetic parameters and clinical outcomes obtained by using higher dosages of drugs for treatment of childhood tuberculosis are needed, and recommended dosages may need to be increased.
Figures
References
-
- Al Dossary, F. S., L. T. Ong, A. G. Correa, and J. R. Starke. 2002. Treatment of childhood tuberculosis with a six month directly observed regimen of only two weeks of daily therapy. Pediatr. Infect. Dis. J. 21:91-97. - PubMed
-
- Biddulph, J. 1990. Short course chemotherapy for childhood tuberculosis. Pediatr. Infect. Dis. J. 9:794-801. - PubMed
-
- Chintu, C., V. Mudenda, S. Lucas, A. Nunn, K. Lishimpi, D. Maswahu, F. Kasolo, P. Mwaba, G. Bhat, H. Terunuma, and A. Zumla. 2002. Lung diseases at necropsy in African children dying from respiratory illnesses: a descriptive necropsy study. Lancet 360:985. - PubMed
-
- Espinal, M. A., A. L. Reingold, G. Perez, E. Camilo, S. Soto, E. Cruz, N. Matos, and G. Gonzalez. 1996. Human immunodeficiency virus infection in children with tuberculosis in Santo Domingo, Dominican Republic: prevalence, clinical findings, and response to antituberculosis treatment. J. Acquir. Immune Defic. Syndr. Hum. Retrovirol. 13:155-159. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
