

Breast lesions: evaluation with US strain imaging--clinical experience of multiple observers
- PMID: 16436810
- PMCID: PMC1761922
- DOI: 10.1148/radiol.2381041336
Breast lesions: evaluation with US strain imaging--clinical experience of multiple observers
Abstract
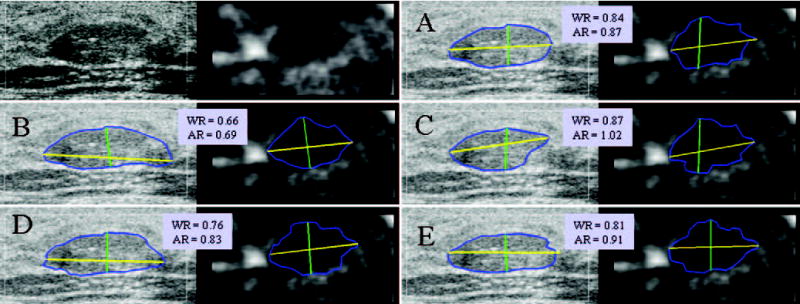
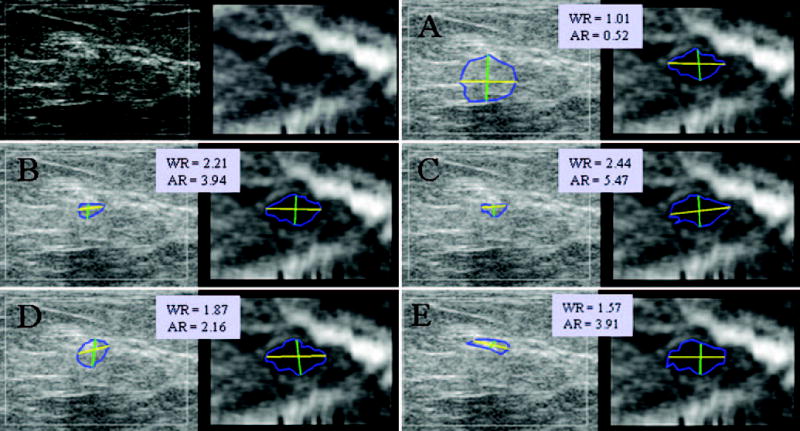
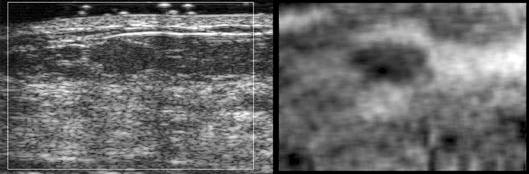
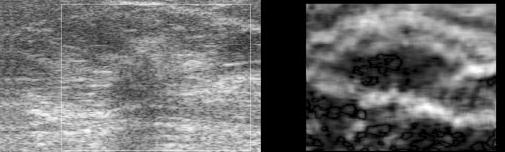
Purpose: To prospectively determine the accuracy of using an ultrasonographic (US) strain imaging technique known as lesion size comparison to differentiate benign from malignant breast lesions.
Materials and methods: Institutional Review Board approval and patient informed consent were obtained for this HIPPA-compliant study. US strain imaging was performed prospectively for 89 breast lesions in 88 patients. Lesions were imaged by using freehand compression and a real-time strain imaging algorithm. Five observers obtained manual measurements of lesion height, width, and area from B-mode and strain images. By using these size measurements, individual observer and group performances were assessed by using the area under the receiver operating characteristic curve (A(z)). The performance of a single size parameter versus that of a combination of size parameters was evaluated by using univariate and multivariate logistic regression.
Results: Group A(z) values showed that width ratio and area ratio yielded the best results for differentiating benign and malignant breast lesions, and they were not statistically different from one another (P = .499). For the group, the performance of area and width, which was superior to that of height and aspect ratio, was statistically significant for all cases (P < .011) except for those that compared area with aspect ratio (P = .118). By using a group threshold of 1.04 for width ratio and 1.13 for area ratio, the sensitivity and specificity of the technique were 96% and 21%, respectively, for width and 96% and 24%, respectively, for area. The best observer achieved a sensitivity of 96% and a specificity of 61% by using the area ratio. For all but one observer, combined size parameters did not improve observer performance (P > .258). Significant interobserver performance variability was observed (P < .001).
Conclusion: Results suggest that US strain imaging has the potential to aid diagnosis of breast lesions. However, manually tracing lesion boundaries for size ratio differentiation in a busy clinical setting did not match the diagnostic performance levels previously reported. Focusing on measurements of lesion width, along with additional observer training or automated processes, may yield a suitable method for routine clinical application.
(c) RSNA, 2006
Figures







References
-
- Anderson WAD. Pathology. St Louis, Mo: Mosby; 1953.
-
- Lerner RM, Huang SR, Parker KJ. Sonoelasticity images derived from ultrasound signals in mechanically vibrated tissues. Ultrasound Med Biol. 1990;16:231–239. - PubMed
-
- Ophir J, Cespedes EI, Ponnekanti H, Yazdi Y, Li X. Elastography: a quantitative method for imaging the elasticity of biological tissues. Ultrason Imaging. 1991;13:111–134. - PubMed
-
- O’Donnell M, Skovoroda A, Shapo B, Emelianov S. Internal displacement and strain imaging using ultrasonic speckle tracking. IEEE Trans Ultrason Ferroelectr Freq Control. 1994;41:314–325.
-
- Skovoroda AR, Emelianov Y, O’Donnell M. Tissue elasticity reconstruction based on ultrasonic displacement and strain images. IEEE Trans Ultrason Ferroelectr Freq Control. 1995;42:747–765.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
