

Galantamine for vascular cognitive impairment
- PMID: 16437493
- PMCID: PMC8406621
- DOI: 10.1002/14651858.CD004746.pub2
Galantamine for vascular cognitive impairment
Update in
-
Galantamine for vascular cognitive impairment.Cochrane Database Syst Rev. 2006 Jan 25;(4):CD004746. doi: 10.1002/14651858.CD004746.pub2. Cochrane Database Syst Rev. 2006. PMID: 23862185
Abstract
Background: Vascular dementia is the second most common form of dementia. Cholinesterase inhibitors modestly improve a broad range of symptoms in some patients with Alzheimer's disease through enhancement of cholinergic neurotransmission. These drugs may also be beneficial in vascular dementia as reductions in acetylcholine and acetyltransferase activity have been reported.
Objectives: To assess the efficacy of galantamine in the treatment of people with vascular cognitive impairment or vascular dementia or "mixed" dementia.
Search strategy: Trials were identified from a search of the Specialized Register of the Cochrane Dementia and Cognitive Improvement Group on 19 April 2005 using the terms: galantamine. galanthamine, reminyl. All major health care databases and many ongoing trial databases within the scope of the group are searched regularly to keep this Register up to date.
Selection criteria: All unconfounded randomised double-blind trials comparing galantamine with placebo were eligible for inclusion.
Data collection and analysis: Two RCTs fulfilling the inclusion criteria were included in this review. Two reviewers independently extracted the data from these two inclusion studies.
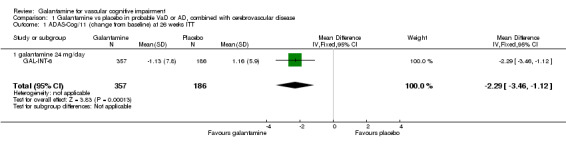
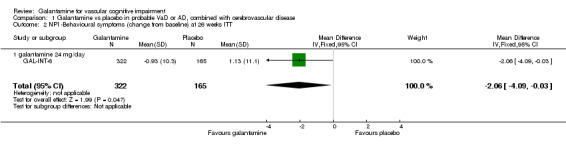
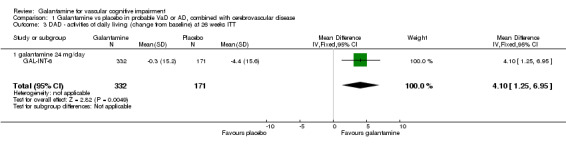
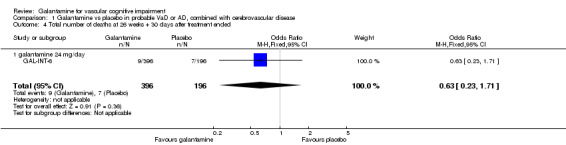
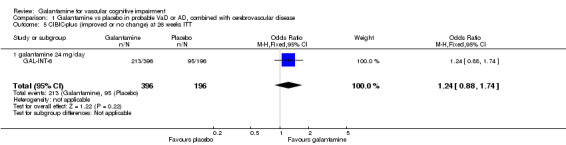
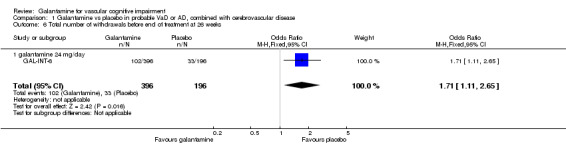
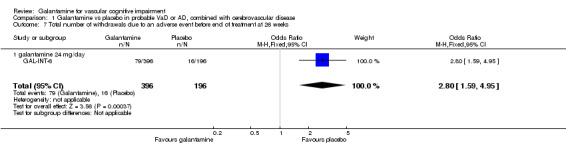
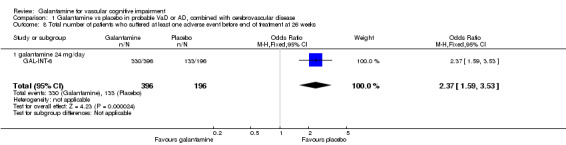
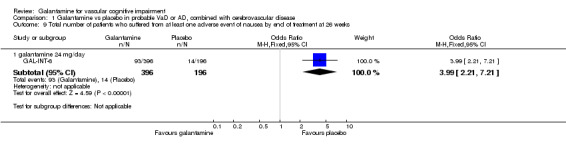
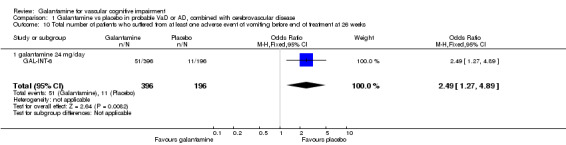
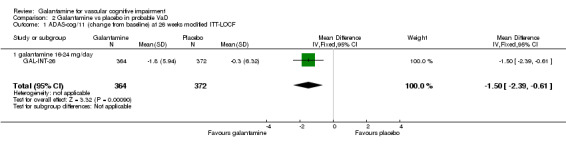
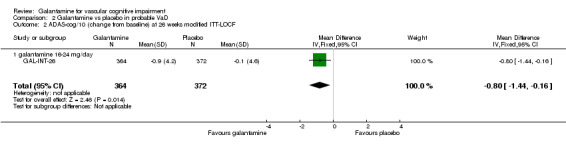
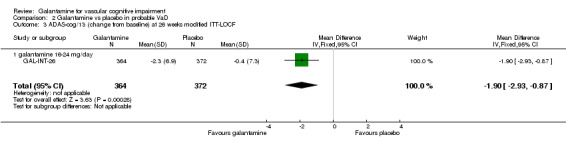
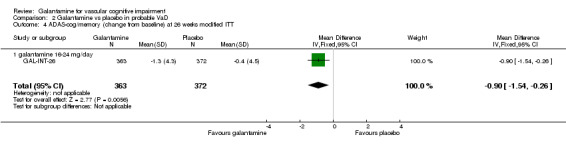
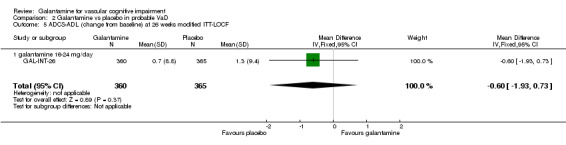
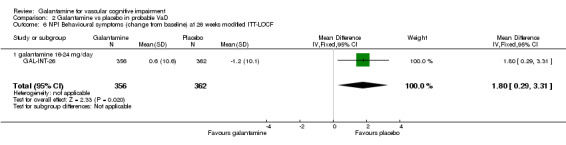
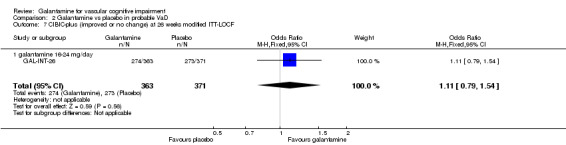
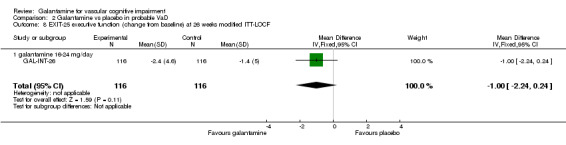
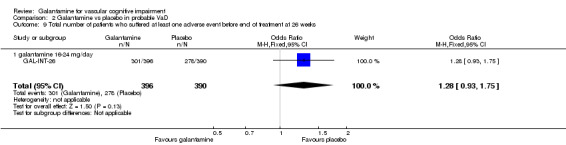
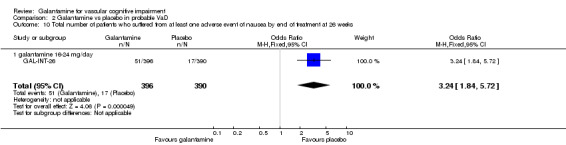
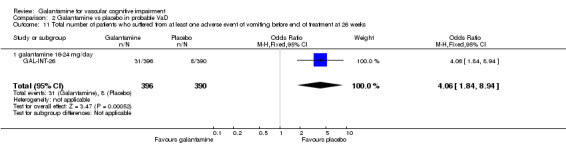
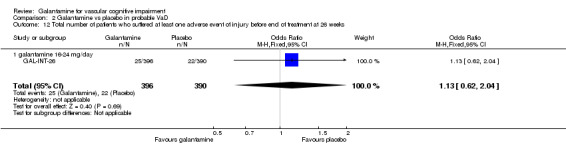
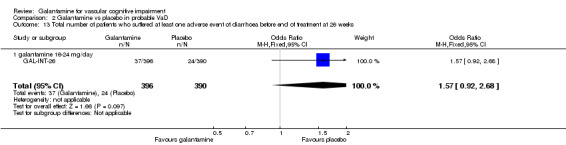
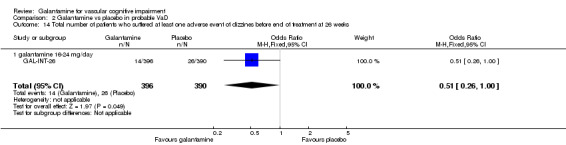
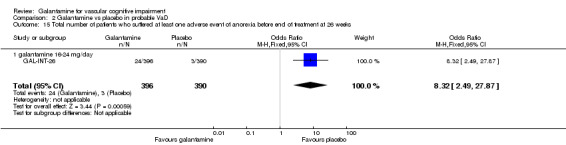
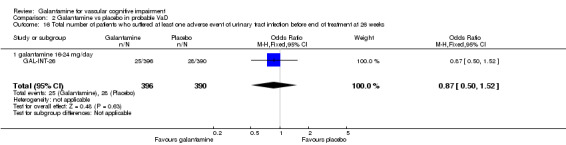
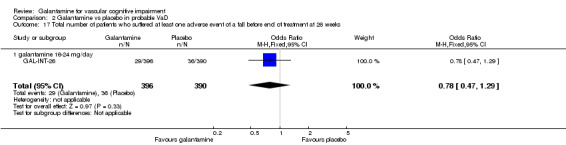
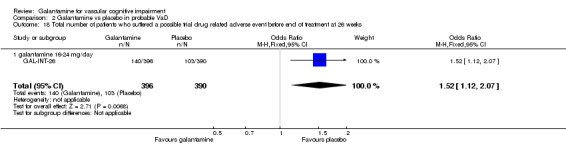
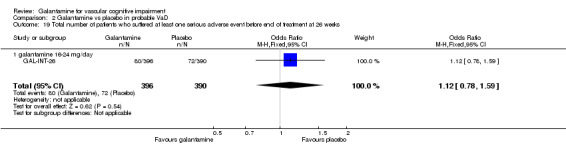
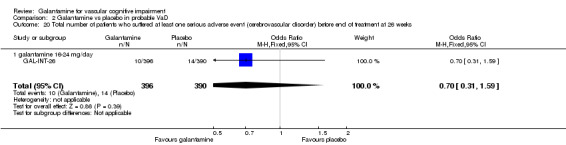
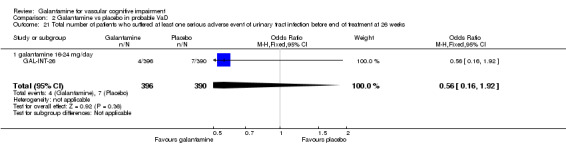
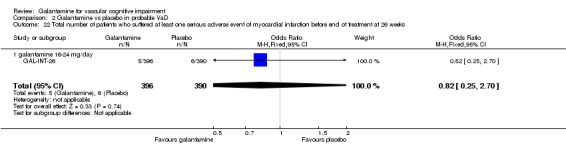
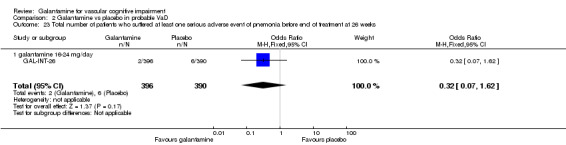
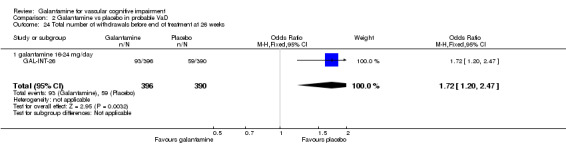
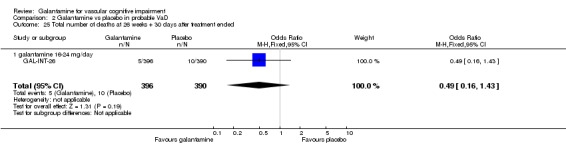
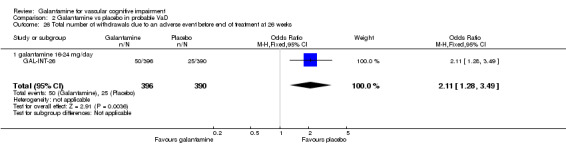
Main results: Two trials employing randomized, double-blind, parallel-group methodology were included. GAL-INT-6 reported sub-group data for a pure population of vascular dementia patients showing no significant differences in Alzheimer's Disease Assessment Scale-cognitive subscale (ADAS-cog/11) and Clinician's Interview-based Impression of Change (CIBIC-plus) when galantamine was compared against placebo. When data combining patients with vascular dementia diagnosed according to recognised criteria with a population of patients with Alzheimer's disease and coincidental radiographic findings of cerebrovascular disease was analysed, statistically significant improvements in cognition (ADAS-cog), global functioning (CIBIC-plus), activities of daily living (DAD) and behaviour (NPI) were noted. In the galantamine treated group, significantly higher numbers of patients dropped out and withdrew due to an adverse event. Limited data was available at the time of publication for a second larger trial (GAL-INT-26) involving patients with vascular dementia diagnosed using standard criteria. Statistically significant benefits favouring galantamine over placebo in assessments of cognition (ADAS-cog/11; p < 0.001) and executive function (Executive Interview, EXIT-25, p = 0.041) were recorded. No differences in outcome in measures of behaviour (Neuropsychiatric Inventory, NPI), daily living (Alzheimer's Disease Cooperative Study-Activities of Daily Living inventory, ADCS-ADL) and global functioning (CIBIC-plus) in this trial were seen.
Authors' conclusions: Limited data were available when considering the impact of galantamine on vascular dementia or vascular cognitive impairment. The data available at the time of review suggest some advantage over placebo in the areas of cognition and executive functioning in one trial but this was not seen in a second trial which included smaller numbers of relevant patients. In both considered trials galantamine produced higher rates of gastrointestinal side-effects. More studies are needed before firm conclusions can be drawn.
Conflict of interest statement
None known.
Figures

References
References to studies included in this review
GAL‐INT‐26 {published and unpublished data}
-
- Anon. GAL‐INT‐26. Johnson and Johnson Pharmceutical Research and Development 26 February 2004.
-
- Auchus AP, Brashear HR, Salloway S, Korczyn AD, Deyn PP, Gassmann‐Mayer C, GAL‐INT‐26 Study Group. Galantamine treatment of vascular dementia: a randomized trial. Neurology 2007;69(5):448‐58. - PubMed
-
- Gassmann‐Mayer C. Email author. E‐mail correspondence from Dr Cristina Gassmann‐Mayer. Email to: R Malouf. Email recipient 24 October 2008.
GAL‐INT‐6 {published data only}
-
- Bullock R, Erkinjuntti T, Lilienfeld S, GAL INT 6 Study Group. Management of patients with Alzheimer's disease plus cerebrovascular disease: 12‐month treatment with galantamine. Dementia and Geriatric Cognitive Disorders 2004;17(1‐2):29‐34. - PubMed
-
- Bullock R, Lilienfeld S. Galantamine shows promising results in Alzheimer's disease with cerebrovascular components and probable vascular dementia (preliminary results). Journal of Neuroscience 2001;187(Suppl 1):S59.
-
- Burke W, Lilienfeld S. Galantamine improves behaviour and relieves caregiver distress in Alzheimer's disease (AD), vascular dementia and AD with cerebrovascular disease. Proceedings of the 8th International Conference on Alzheimer's Disease and Related Disorders; 2002 July 20‐25, Stockholm, Sweden 2002:Abstract No 428. 2002.
-
- Erkinjuntti T. Broad therapeutic benefits in patients with probable vascular dementia or Alzheimer's disease with cerebrovascular disease after treatment with galantamine. European Journal of Neurology 2002;9(5):545. - PubMed
-
- Erkinjuntti T, Gauthier S, Bullock R, Kurz A, Hammond G, Schwalen S, et al. Galantamine treatment in Alzheimer's disease with cerebrovascular disease: Responder analyses from a randomized, controlled trial (GAL‐INT‐6). Journal of Psychopharmacology 2008;22(7):761‐8. - PubMed
References to studies excluded from this review
Senanarong 2004 {published data only}
-
- Senanarong V, Poungvarin N, Phanthumchinda K, Tavichachart N, Chankrachang S, Praditsuwan R, et al. Tolerability study of galantamine in possible Alzheimer's disease with or without cerebrovascular disease; a slow‐titration regimen in Thai patients. 8th Congress of the European Federation of the Neurological Sciences. Paris, France. September 4‐7. 2004.
-
- Thavichachart N, Phanthumchinda K, Chankrachang S, Praditsuwan R, Nidhinandana S, Senanarong V, et al. Efficacy study of galantamine in possible Alzheimer's disease with or without cerebrovascular disease; a slow‐titration regimen in Thai patients. 8th Congress of the European Federation of the Neurological Sciences. Paris, France. September 4‐7. 2004.
Small 2003 {published data only}
-
- Small GW, Ekinjuntti T, Kurz A, Lilienfeld S. Galantamine in the treatment of cognitive decline in patients with vascular dementia or Alzheimer's disease with cerebrovascular disease. CNS Drugs 2003;17:905‐14. - PubMed
Additional references
Chui 1992
-
- Chui H, Victoroff J, Margolin D, Jagust W, Shankle R, Katzman R. Criteria for the diagnosis of ischemic vascular dementia proposed by the State of California Alzheimer's Disease Diagnostic and Treatment Centers. Neurology 1992;42(3 Part 1):473‐80. - PubMed
Cummings 1993
-
- Cummings JL. Frontal‐subcortical circuits and human behavior. Archives of Neurology 1993;50(8):873‐80. - PubMed
Cummings 1994
-
- Cummings JL, Mega M, Gray K, Rosenberg‐Thompson S, Carusi DA, Gornbein J. The Neuropsychiatric Inventory: comprehensive assessment of psychopathology in dementia. Neurology 1994;44:2308‐14. - PubMed
Erkinjuntti 2000
-
- Erkinjuntti T, Inzitari D, Pantoni L, Wallin A, Scheltens P, Rockwood K, et al. Research criteria for subcortical vascular dementia in clinical trials. Journal of Neural Transmission 2000;59(Supplement):23‐30. - PubMed
Galasko 1997
-
- Galasko D, Bennett D, Sano M, Ernesto C, Thomas R, Grundman M, et al. An inventory to assess activities of daily living for clinical trials in Alzheimer's disease. The Alzheimer's Disease Cooperative Study. Alzheimer's Disease and Associated Disorders 1997;11 Suppl 2:S33‐9. - PubMed
Gelinas 1999
-
- Gelinas I, Gauthier L, McIntyre, M. Development of a functional measure for persons with Alzheimer's disease: the Disability Assessment for Dementia. American Journal of Occupational Therapy 1999;53:471‐81. - PubMed
Knopman 1994
-
- Knopman DS, Knapp MJ, Gracon SI, Davis CS. The Clinician Interview Based Impression (CIBI): a clinician's global change rating scale in Alzheimer's disease. Neurology 1994;44:2315‐21. - PubMed
Lilienfeld 2002
Malouf 2004
McKhann 1984
-
- McKhann G, Drachman D, Folstein M, Katzman R, Price D, Stadlan EM. Clinical diagnosis of Alzheimer's disease: report of the NINCDS‐ADRDA Work Group under the auspices of Department of Health and Human Sciences Task Force on Alzheimer's disease. Neurology 1984;34:939‐44. - PubMed
MRC CFAS 2001
-
- MRC CFAS, Neuropathology Group of the Medical Research Council Cognitive Function and Ageing Study (MRC CFAS). Pathological correlates of late‐onset dementia in a multicentre, community‐based population in England and Wales. The Lancet 2001;357:169‐75. - PubMed
O'Brien 2000
-
- O'Brien J, Perry R, Barber R, Gholkar A, Thomas A. The association between white matter lesions on magnetic resonance imaging and noncognitive symptoms. Annals of the New York Academy of Sciences 2000;903:482‐9. - PubMed
O'Brien 2003
-
- O'Brien JT, Erkinjuntti T, Reisberg B, Roman G, Sawada T, Pantoni L, et al. Vascular cognitive impairment. The Lancet Neurology 2003;2:89‐98. - PubMed
Perry 1997
-
- Perry E, Kay DW. Some developments in brain ageing and dementia. British Journal of Biomedical Science 1997;54(3):201‐15. - PubMed
Perry 2005
-
- Perry E, Ziabreva I, Perry R, Aarsland D, Ballard C. Absence of cholinergic deficits in "pure" vascular dementia. Neurology 2005;64:132‐3. - PubMed
Pohjasvaara 2003
-
- Pohjasvaara T, Mantyla R, Ylikoski R, Kaste M, Erkinjuntti T. Clinical features of MRI‐defined subcortical vascular disease. Alzheimer's Disease and Associated Disorders 2003;17(4):236‐42. - PubMed
Roman 1993
-
- Roman G, Tatemichi T, Erkinjuntti T, Cummings JL, Masdeu JC, Garcia JH, et al. Vascular dementia: diagnostic criteria for research studies. Report of the NINDS‐AIREN International Workshop. Neurology 1993;43(2):250‐60. - PubMed
Rosen 1984
-
- Rosen WG, Mohs RC, Davis KL. A new rating scale for Alzheimer's disease. American Journal of Psychiatry 1984;141(11):1356‐64. - PubMed
Royall 1992
-
- Royall DR, Mahurin RK, Gray KF. Bedside assessment of executive cognitive impairment: the executive interview. Journal of the American Geriatrics Society 1992;40(12):1221‐6. - PubMed
Toghi 1996
-
- Toghi H, Abe T, Kimura M, Saheki M, Takahashi S. Cerebrospinal fluid acetylcholine and choline in vascular dementia of Binswanger and multiple small infarcts types as compared with Alzheimer‐type dementia. Journal of Neural Transmission 1996;103:1211‐20. - PubMed
WHO 1992
-
- World Health Organization. International classification of diseases, 10th revision. Geneva: World Health Organization, 1992.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous