

Learning curve of laparoscopy-assisted distal gastrectomy with systemic lymphadenectomy for early gastric cancer
- PMID: 16437724
- PMCID: PMC4725181
- DOI: 10.3748/wjg.v11.i47.7508
Learning curve of laparoscopy-assisted distal gastrectomy with systemic lymphadenectomy for early gastric cancer
Abstract
Aim: To evaluate the nature of the "learning curve" for laparoscopy-assisted distal gastrectomy (LADG) with systemic lymphadenectomy for early gastric cancer.
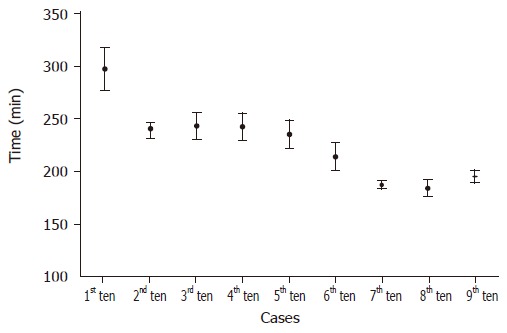
Methods: The data of 90 consecutive patients with early gastric cancer who underwent LADG with systemic lymphadenectomy between April 2003 and November 2004 were reviewed. The 90 patients were divided into 9 sequential groups of 10 cases in each group and the average operative time of these 9 groups were determined. Other learning indicators, such as transfusion requirements, conversion rates to open surgery, postoperative complication, time to first flatus, and postoperative hospital stay, were evaluated.
Results: After the first 10 LADGs, the operative time reached its first plateau (230-240 min/operation) and then reached a second plateau (<200 min/operation) for the final 30 cases. Although a significant improvement in the operative time was noted after the first 50 cases, there were no significant differences in transfusion requirements, conversion rates to open surgery, postoperative complications, time to first flatus, or postoperative hospital stay between the groups.
Conclusion: Based on operative time analysis, this study show that experience of 50 cases of LADG with systemic lymphadenectomy for early gastric cancer is required to achieve optimum proficiency.
Figures
References
-
- Polkowski M, Palucki J, Wronska E, Szawlowski A, Nasierowska-Guttmejer A, Butruk E. Endosonography versus helical computed tomography for locoregional staging of gastric cancer. Endoscopy. 2004;36:617–623. - PubMed
-
- Ishigami S, Yoshinaka H, Sakamoto F, Natsugoe S, Tokuda K, Nakajo A, Matsumoto M, Okumura H, Hokita S, Aikou T. Preoperative assessment of the depth of early gastric cancer invasion by transabdominal ultrasound sonography (TUS): a comparison with endoscopic ultrasound sonography (EUS) Hepatogastroenterology. 2004;51:1202–1205. - PubMed
-
- Hayes N, Karat D, Scott DJ, Raimes SA, Griffin SM. Radical lymphadenectomy in the management of early gastric cancer. Br J Surg. 1996;83:1421–1423. - PubMed
-
- Maruyama K, Sasako M, Kinoshita T, Sano T, Katai H. Can sentinel node biopsy indicate rational extent of lymphadenectomy in gastric cancer surgery? Fundamental and new information on lymph-node dissection. Langenbecks Arch Surg. 1999;384:149–157. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
