

Spinal lumbar synovial cysts. Diagnosis and management challenge
- PMID: 16440202
- PMCID: PMC3233964
- DOI: 10.1007/s00586-005-0009-4
Spinal lumbar synovial cysts. Diagnosis and management challenge
Abstract
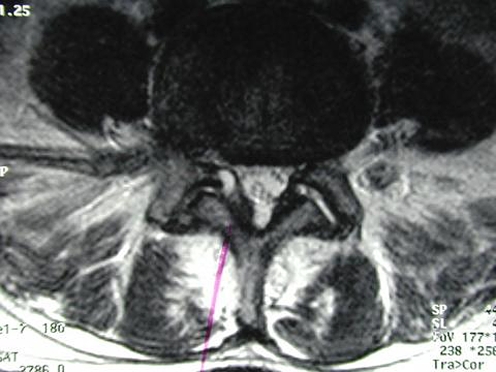
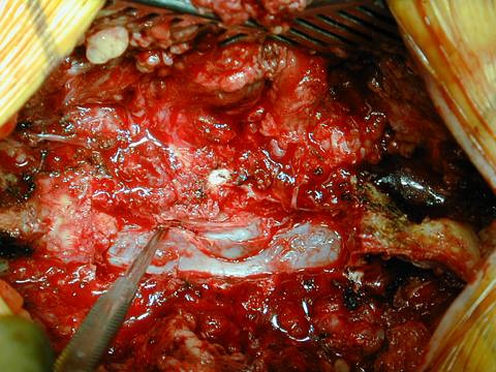
Sophisticated and newer imaging capabilities have resulted in increased reporting and treatment options of spinal lumbar synovial cysts (LSS). Most of the patients with lumbar cysts tend to be in their sixth decade of life with a slight female predominance. The incidence of LSS is thought to be less than 0.5% of the general symptomatic population. They may be asymptomatic and found incidentally or the epidural growth of cysts into the spinal canal can cause compression of neural structures and hence associated clinical symptoms. Most of the symptomatic LSS patients present with radicular pain and neurological deficits. Spinal synovial cysts are commonly found at L4-5 level, the site of maximum mobility. They may be unilateral or bilateral and at one or multilevel. MRI is considered the tool of choice for its diagnosis. The etiology of LSS is still unclear, but underlying spinal instability, facet joint arthropathy and degenerative spondylolisthesis has a strong association for worsening symptoms and formation of spinal cysts. Synovial cysts resistant to conservative therapy should be treated surgically. Resection and decompression with or without fusion and instrumentation remains an appropriate option. Synovial cysts may recur following surgery. The optimal approach for patients with juxtafacet LSS remains unclear. The best surgical treatment option for each particular individual should be tailored depending upon the symptoms, radiological findings and other co morbidities.
Figures


References
-
- Baker WM. Formation of synovial cysts in connection with joints. St. Bartholomews Hospital Reports. 1885;21:177–190.
-
- Baker WM. On the formation of synovial cysts in the leg in connection with disease of the knee-joint 1877. Clin Orthop. 1994;299:2–10. - PubMed
-
- Bandiera S, et al. Hemorrhagic synovial lumbar cyst: a case report and review of the literature. Chir Organi Mov. 1999;84.2:197–203. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
