

doi: 10.1111/j.1469-7580.2006.00524.x.
Morphogenesis of the second pharyngeal arch cartilage (Reichert's cartilage) in human embryos
Affiliations
- PMID: 16441562
- PMCID: PMC2100189
- DOI: 10.1111/j.1469-7580.2006.00524.x
Item in Clipboard
Morphogenesis of the second pharyngeal arch cartilage (Reichert's cartilage) in human embryos
J Anat.
2006 Feb.
Abstract
This study was performed on 50 human embryos and fetuses between 7 and 17 weeks of development. Reichert's cartilage is formed in the second pharyngeal arch in two segments. The longer cranial or styloid segment is continuous with the otic capsule; its inferior end is angulated and is situated very close to the oropharynx. The smaller caudal segment is in contact with the body and greater horn of the hyoid cartilaginous structure. No cartilage forms between these segments. The persistent angulation of the inferior end of the cranial or styloid segment of Reichert's cartilage and its important neurovascular relationships may help explain the symptomatology of Eagle's syndrome.
Figures
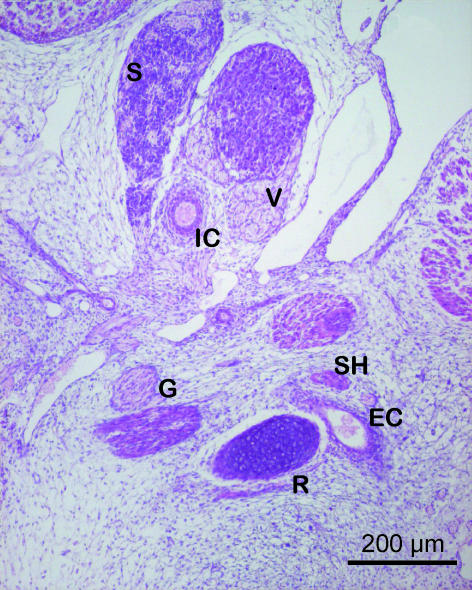
Human embryo GV-6 (22 mm CRL). Frontal section. Haematoxylin–eosin staining. Cranial segment of Reichert's cartilage (R), connected with the external carotid artery (EC), lying between Reichert's cartilage and the stylohyoid muscle (SH). The vasculonervous elements of the retrostyloid space are dorsal to Reichert's cartilage: glossopharyngeal nerve (G), vagus nerve (V), internal carotid artery (IC), superior cervical ganglion (S).
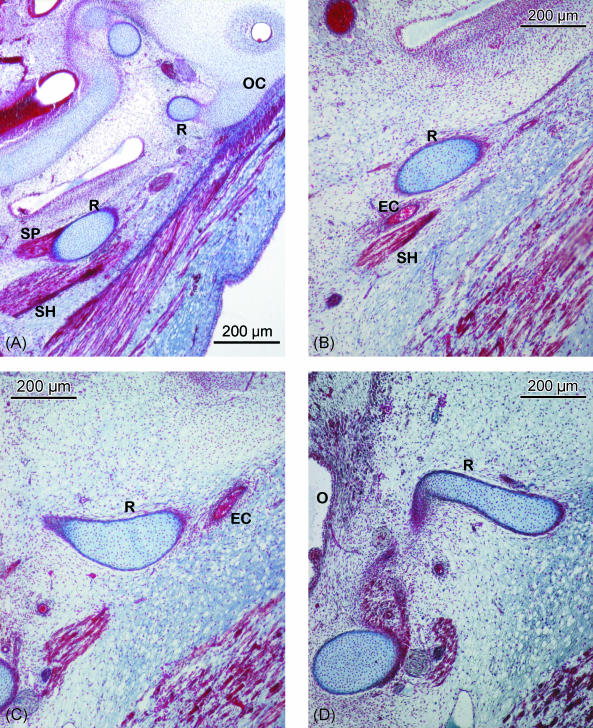
(A–E) Human embryo BR-4 (28 mm CRL). Frontal sections. Azocarmine staining. (A) Hooked superior end of Reichert's cartilage (R) showing its continuity with the otic capsule (OC); due to the caudoventromedial direction of the cartilage, this is also sectioned caudally at the origin of the stylopharyngeal (SP) and stylohyoideal (SH) muscles. (B) The external carotid artery (EC) passing between Reichert's cartilage (R) and the stylohyoid muscle (SH). (C) The start of the angulation of the inferior end of the cranial segment of Reichert's cartilage (R). External carotid artery (EC). (D) Change in direction of the lower end of the cranial segment of Reichert's cartilage (R) orientated towards the oropharynx (O). (E) Mesenchymal condensation (MC), which continues caudally to the cranial segment of Reichert's cartilage clearly distinguished from the cartilage of the third pharyngeal arch (greater horn of the hyoid cartilaginous structure) (GR). Glossopharyngeal nerve (G). Hypoglossal nerve (H). (F) Human embryo BR-2 (28.5 mm CRL). Frontal section. Haematoxylin–eosin staining. Caudal or hyoid segment of Reichert's cartilage (RR) in contact with the body (B) and the greater horn (GR) of the hyoid cartilaginous structure.
(A–E) Human embryo BR-4 (28 mm CRL). Frontal sections. Azocarmine staining. (A) Hooked superior end of Reichert's cartilage (R) showing its continuity with the otic capsule (OC); due to the caudoventromedial direction of the cartilage, this is also sectioned caudally at the origin of the stylopharyngeal (SP) and stylohyoideal (SH) muscles. (B) The external carotid artery (EC) passing between Reichert's cartilage (R) and the stylohyoid muscle (SH). (C) The start of the angulation of the inferior end of the cranial segment of Reichert's cartilage (R). External carotid artery (EC). (D) Change in direction of the lower end of the cranial segment of Reichert's cartilage (R) orientated towards the oropharynx (O). (E) Mesenchymal condensation (MC), which continues caudally to the cranial segment of Reichert's cartilage clearly distinguished from the cartilage of the third pharyngeal arch (greater horn of the hyoid cartilaginous structure) (GR). Glossopharyngeal nerve (G). Hypoglossal nerve (H). (F) Human embryo BR-2 (28.5 mm CRL). Frontal section. Haematoxylin–eosin staining. Caudal or hyoid segment of Reichert's cartilage (RR) in contact with the body (B) and the greater horn (GR) of the hyoid cartilaginous structure.
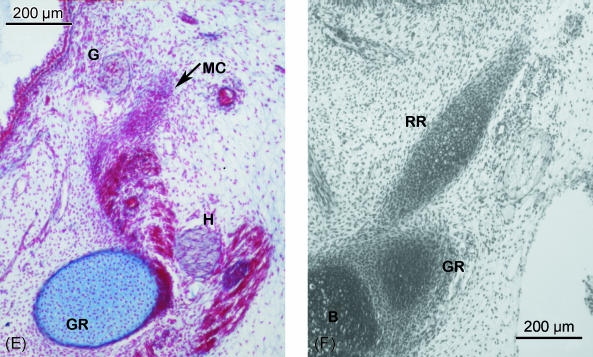
(A–C) Human fetus JR-1 (55 mm CRL). Transverse sections. Azocarmine staining. (A) Superior end of the cranial segment of Reichert's cartilage (R), joined to the otic capsule (OC) and forming with this the vertical portion of the facial canal. Facial nerve (F). (B) Reichert's cartilage (R) is related to the tympanic part of the temporal bone (T) that separates it from Meckel's cartilage (M). The stylopharyngeal muscle (SP) originates in Reichert's cartilage; dorsally is the posterior belly of the digastric muscle (D). (C) Angulated inferior portion of the cranial segment of Reichert's cartilage (R), situated dorsal to the mandibular angle (MA). The angulated end touches the pharyngeal wall (PH). Greater horn of the hyoid cartilaginous structure (GR). Meckel's cartilage (M). (D) Human fetus Bu-14 (72 mm CRL). Transverse section. Haematoxylin–eosin staining. Inferior portion of the cranial segment of Reichert's cartilage (R). This presents a clear angulation dorsomedial to the mandibular angle (MA). The glossopharyngeal nerve (G) close to the stylopharyngeal muscle (SP) and with the angulated end of Reichert's cartilage (R). Meckel's cartilage (M). Oropharynx (O). (E) Human fetus Be-101 (65 mm CRL). Frontal section. Azocarmine staining. Caudal segment of Reichert's cartilage (RR) that will form the lesser horn of the hyoid cartilaginous formation, situated between the body (B) and the greater horn (GR). Hypoglossal nerve (H). Hyoglossus muscle (HM). Lingual artery (LA). Submandibular gland (SG). (F) Human fetus JR-1 (55 mm CRL). Azocarmine staining. Transverse section at the lateral suprahyoid region where Reichert's cartilage does not form. The hyoglossus muscle (HM) originates in the greater horn (GR) of the hyoid cartilaginous formation. The hypoglossus nerve (H) and the intermediate tendon of the digastric muscle (DI) run laterally to the hyoglossus muscle. The submandibular gland (SG) lies laterally to these structures.
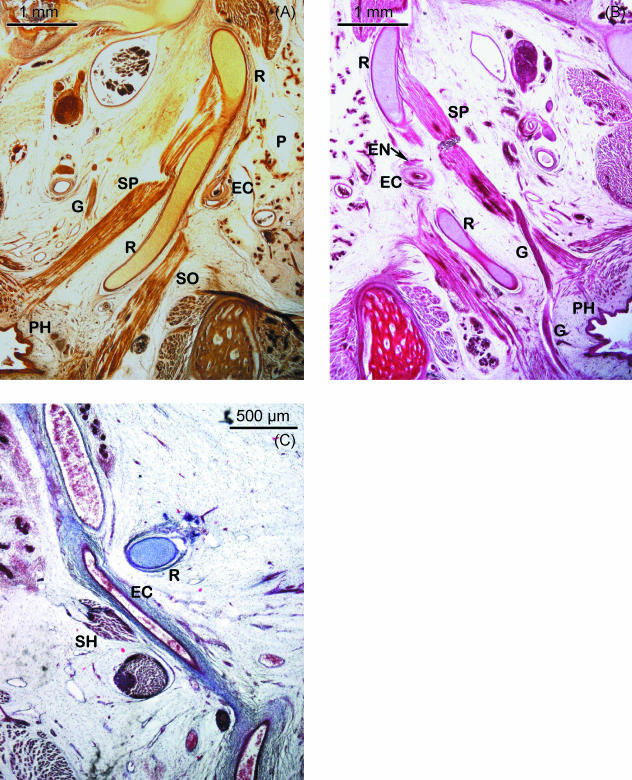
(A,B) Human fetus Be-608 (90 mm CRL). Transverse section. Bielschowsky staining. (A) Cranial segment of Reichert's cartilage (R) that presents a less pronounced angulation. Lateral to the cartilage, the external carotid artery (EC), the parotid gland (P) and the styloglossus muscle (SO) can be observed. The stylopharyngeal muscle (SP) and the glossopharyngeal nerve (G) are medial to the cartilage. Pharynx (PH). (B) Haematoxylin–eosin staining. Relationships between the cranial segment of Reichert's cartilage (R) and the external carotid artery (EC) and the external carotid nerves (EN) that surround it and with the glossopharyngeal nerve (G) situated between the end of the cartilage and the pharynx (PH). Stylopharyngeal muscle (SP). (C) Human fetus JR-6 (80 mm CRL). Frontal section. Azocarmine staining. The external carotid artery (EC) can be observed in the space formed between Reichert's cartilage (R) and the stylohyoid muscle (SH) situated laterally.
References
-
- Abramovich A. Embriología de la región maxilofacial. Buenos Aires: Editorial Médica Panamericana; 1997.
-
- Arnould G, Tridon P, Laxenaire M, Picard L, Weber M, Masingue M. Appareil stylo-hyoïdien et malformations de la charnière occipito-vertébrale. A propos de cinq observations. Rev Otoneuroophtalmol. 1969;41:190–195. - PubMed
-
- Avery JK. Oral Development and Histology. 3. Stuttgart: Georg Thieme Verlag; 2002.
-
- Babad MS. Eagle's syndrome caused by traumatic fracture of a mineralized stylohyoid ligament. Literature review and a case report. Cranio. 1995;13:188–192. - PubMed
-
- Baddour HM, McAnear JT, Tilson HB. Eagle's syndrome. Report of a case. Oral Surg Oral Med Oral Pathol. 1978;46:486–494. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
